All published articles of this journal are available on ScienceDirect.

Pediatric Pseudotumor Cerebri: Epidemiological Features.
Abstract
Objective:
The purpose was to study the epidemiological and clinical features of Pediatric Pseudotumor Cerebri; we especially evaluated age, sex, sexual maturity, weight, symptoms, duration of the episode, visual acuity, correlation with systemic diseases or drugs.
Methods:
We investigated a population of 40 children (80 eyes), aged between 2 and 18 years, that referred to our Centre (Città della Salute e della Scienza di Torino - presidio Ospedale Regina Margherita) from 2000 to 2018.
All the patients were monitored with visual field exam, fundus exam and Frisen classification, pupillary reflexes, best corrected visual acuity, orthoptic exam.
Then, the demographic characteristics, BMI (body max index) and weight changes, the correlation with systemic diseases or drugs, the Relative Afferent Pupillary Defect (RAPD), the VI cranial nerve deficit, the time required for the diagnosis, the modality of onset, the correlation between diagnosis delay and best corrected visual acuity, the resolution time and the probability of recurrence were studied.
Results:
We observed 2 age peaks in our population, one consisting of adolescents (aged between 11 and 14 years) and one consisting of younger children aged between 4 and 7 years, with a statistically significant correlation between age and BMI.
The deficit of the VI cranial nerve and the diplopia were resolved within the first month, despite the longer time of resolution of the papilledema.
Headache was the main onset symptom, but after reclassifying onset symptoms per weight classes, in overweight children, we found an increased variability of symptoms (dizziness, postural instability, photophobia, nausea, vomit, strabism and diplopia, visual fogging, drowsiness, irritability). Moreover, we found only one totally asymptomatic case, during a routine visit, in a 6 years old overweight child with Down syndrome.
Conclusion:
The Pediatric Pseudotumor Cerebri is, even nowadays, a little known pathology.
To provide a correct diagnostic assessment, it will be imperative to recollect the epidemiological features of this disease.
1. INTRODUCTION
The Pediatric Idiopathic Intracranial Hypertension or Pseudotumor Cerebri is a clinical condition characterized by a raised intracranial pressure and papilledema in the absence of clinical, biochemical and neurological evidences of masses, structural lesions, infections or vascular brain anomalies, in a pediatric patient.
Although it predominantly affects young adult obese women, it can be diagnosed in children of all ages, and in these populations, it has distinguishing characteristics.
It has an incidence of between 12 and 28 per 100,000 adult persons per year in Europe and the USA, while in children, the annual incidence is between 0.47 (Germany) and 1,2 (Croatia) per 100,000 persons per year [1, 2].
The diagnostic criteria were written for the first time by Dandy in 1937; in 1985, Smith proposed the “Dandy's modified criteria” listed below:
- papilledema, signs and symptoms of raised intracranial pressure (headache, nausea, vomit, etc.);
- normal neurologic examination except for cranial nerve abnormalities;
- Neuroimaging: normal brain parenchyma without evidence of hydrocephalus, mass, or structural lesion on CT – cranial tomography - (while nowadays, the gold standard is MRI – magnetic resonance imaging -);
- Elevated lumbar puncture opening pressure (> 25 cm H2O in adults) with normal biochemical composition.
Nowadays, the same authors have established a lumbar pressure ≥ 28 cm H2O as diagnostic criteria in children younger than 8 years old [3-6].
The precise etiology of Pseudotumor Cerebri is largely unknown, despite that much clinical investigation and basic science researches have been conducted [7-9].
Many researchers are supporting the theory that, in the Idiopathic Intracranial Hypertension syndrome, the reduced absorption of the cerebrospinal fluid is due to an obstacle at the level of the arachnoid villi reabsorption and flux [8, 9].
Several exogenous factors have been proved to be the cause of Secondary Pseudotumor, such as corticosteroid use, human growth hormone use, tetracycline use, excessive vitamin A use, etc., as well as several endocrinological and metabolic diseases (obesity, Turner syndrome, hyperaldosteronism, renal diseases) [10-16].
Despite this, the pathophysiological mechanism of the Pseudotumor Cerebri, and especially the Pediatric one, which is different from the adult form because it is unrelated to obesity and hormonal factors, remains unknown.
The purpose of our research was to study the epidemiological and clinical features of Pediatric Pseudotumor Cerebri, to better define the characteristics of the population and to facilitate the diagnosis.
We investigated a population of 40 children (80 eyes), aged between 2 and 18 years, that referred to our Centre (Città della Salute e della Scienza di Torino - presidio Ospedale Regina Margherita) from 2000 to 2018.
2. MATERIALS AND METHODS
We enrolled 40 patients (80 eyes) with the diagnosis of Pseudotumor Cerebri, who met Dandy's modified criteria, aged from 2 to 18 years old; 40 patients included 20 girls and 20 boys, who were monitored in our Hospital (Città della Salute e della Scienza di Torino - presidio Ospedale Regina Margherita) from 2000 to 2018.
We excluded 21 children with intracranial hypertension due to brain venous thrombosis, 13 children with Chiari diseases, 1 child with Miller Fisher syndrome and 15 children with Pseudopapilledema due to optic nerve drusen.
During the first visit, at presentation, i.e. at time 0, we evaluated all the children for the following factors:
- Age, sex and grading on the Tanner scale
- General, familiar and ophthalmic anamnesis
- BMI (body max index) and latest changes in weight
- Duration of the episode
- Symptoms and onset
- Orthoptic exam
- Best corrected visual acuity
- Pupillary reflexes
- Slit lamp exam of the anterior and posterior segment
- Frisen classification (conducted always by the same expert, G.D.)
- Brain magnetic resonance imaging (MRI)
- Lumbar puncture with liquor analysis
- Visual field exam (Humprey or Goldmann perimeter, depending on child collaboration).
The Tanner scale is an objective classification system used to document and track the development and sequence of secondary sex characteristics of children during puberty. The scale defines physical measurements of development based on external sex characteristics, such as the size of the breasts, genitals, testicular volume and development of pubic hair.
The Frisen classification is the most frequently used system for ranking papilledema severity; it describes clinical stages of optic disk swelling (grade 0-5), evaluating a nasal blur, a temporal blur, a peripheral obscuration of major vessel segments by swollen axons, an elevation of the whole optic nerve head and a protrusion of the optic nerve head as a dome.
All the patients were monitored with visual field exam, fundus exam and Frisen classification, pupillary reflexes, best corrected visual acuity, orthoptic exam, at time 1 (1 week after the onset), at time 2 (2 weeks after the onset), at time 3 (1 month after the onset), at time 4 (3 months after the onset), at time 5 (6 months after the onset), at time 6 (9 months after the onset), and at time 7 (1 year after the onset).
All the patients were treated with acetazolamide 10 mg/Kg/die, supplemented with bicarbonates. 32 children were also treated with dexamethasone 2 mg per 3 doses, 10 children were subjected to lumbar punctures and 4 children were subjected to ventriculo peritoneal derivation. 21 patients were also put on a diet (if BMI>25).
Then, we studied:
-The demographic characteristics;
- BMI and weight changes;
- Correlation with systemic diseases or drugs;
- Best corrected visual acuity at time 0, time 3 and time 5;
- Visual field exam at time 0, time 3 and time 5;
- Frisen classification at time 0, time 3 and time 5;
- Relative afferent pupillary defect (RAPD), VI cranial nerve deficit, diplopia at time 0;
- Time required for the diagnosis, modality of onset, correlation between diagnosis delay and best corrected visual acuity and MD (mean defect in visual field exam) at time 0; correlation between diagnosis delay and response to therapy; correlation between diagnosis delay and Frisen classification at time 0;
- Resolution time and the probability of recurrence;
- Correlation between MD and Frisen classification at time 0, time 3 and time 5.
We used the Pearson test to calculate the correlation coefficient.
3. RESULTS
3.1. Sex
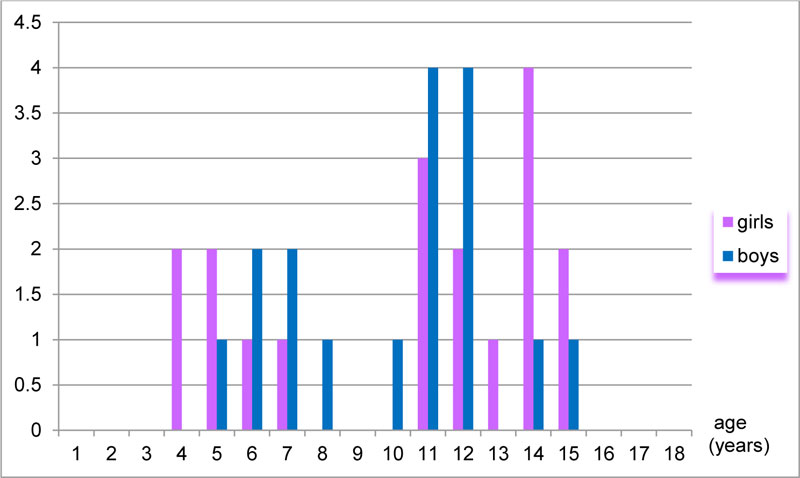
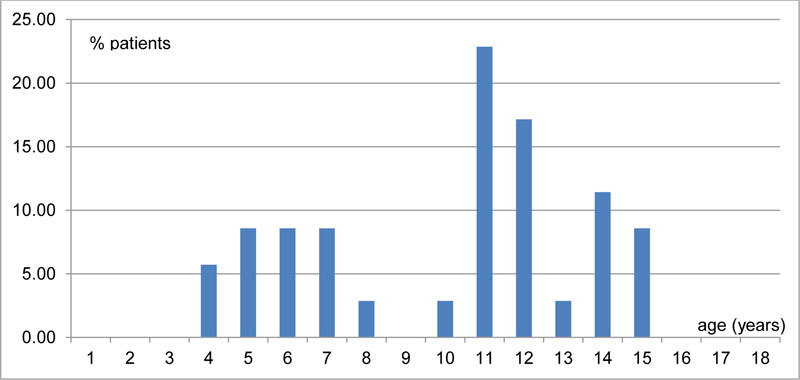
We observed 2 age peaks in our population, one consisting of adolescents and one consisting of younger children, aged between 4 and 7 years. (Fig. 1, 2)
The adolescent group can be considered in association with the pubertal development and the related weight gain, as widely demonstrated in the literature [17].
With advancing age, an even more precocious menarche is being observed, related to an increasing number of younger obese children, in addition to general economic prosperity in the Western World [18, 19].
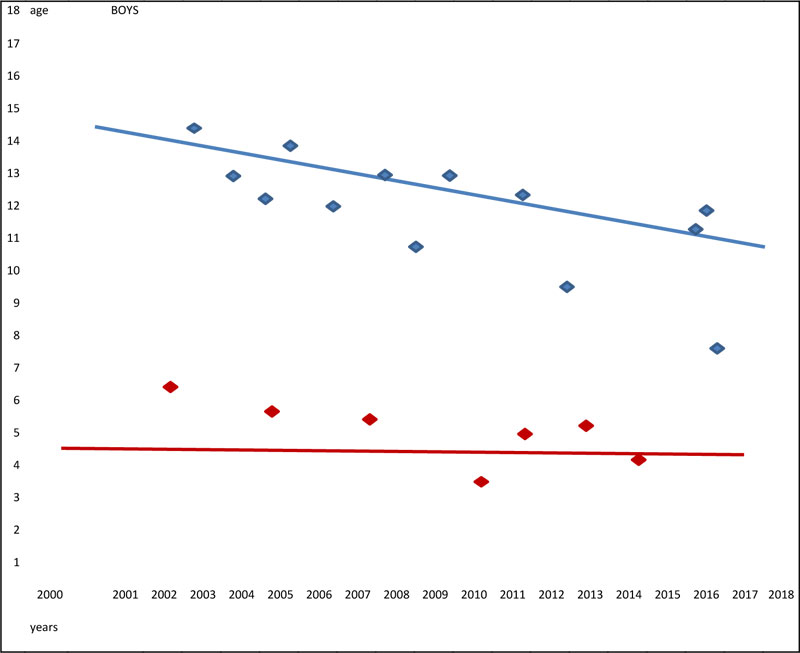
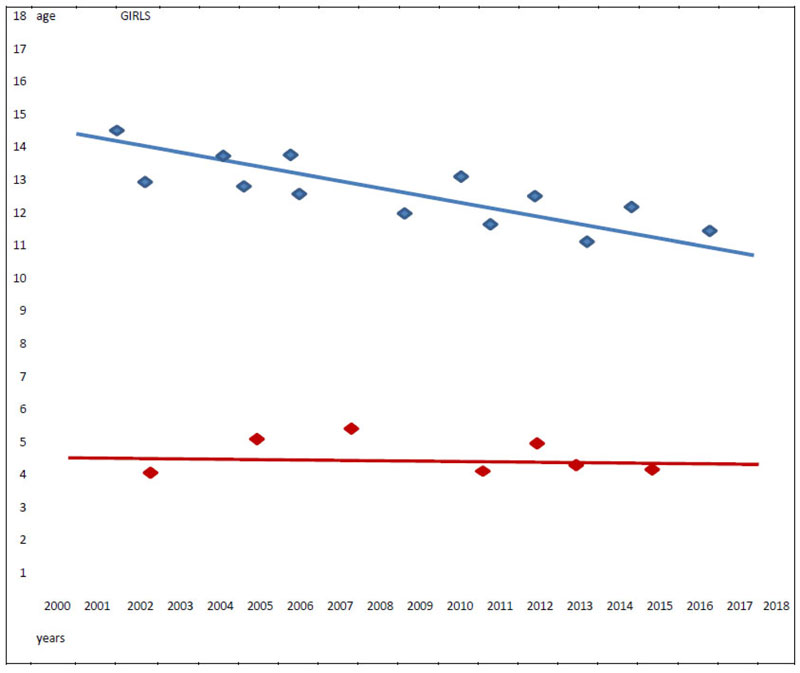
In our population sample, we observed that while the younger age group remained stable over time in terms of numbers of elements and age of onset, the adolescent group has anticipated over the years the age of onset; this result was consistent for both males and females. (Fig. 3 and 4)
3.2. Weight
We calculated the BMI (body max index) (weight - kg - / height - m2 -) using the “BMI Z-scores CDC 2000 growth charts”.
The mean BMI at the onset was 26.773 (sd. 6.621). 19.51% of the population sample had a BMI greater than 30. (Fig. 5)
41.463% of the population sample experienced an increase in weight in the last month. One patient had a weight loss of 2 kg in the latest 15 days instead.
We calculated a p-correlation of 0.219 (p<0.005) between age and BMI, resulting in lower BMI in younger children.
Then, we divided our patients into two groups, according to the presence of pubertal development (menarche or hairiness, breast and testicular size development, on the basis of the Tanner scale) [20].
At this point, the first group without pubertal development had a mean age of 6.611 years old and 44.44% of the population was female. BMI mean was 25.888 (sd 4.788) and nostatistically significant p (p<0.005) was observed between age and BMI. The second group, with pubertal development, had a mean age of 13.412 years old, in which 58.33% were females; the mean BMI was 27.561 (sd 5.448) and we calculated a statistically significant p (0.450) (p<0.005) between age and BMI.
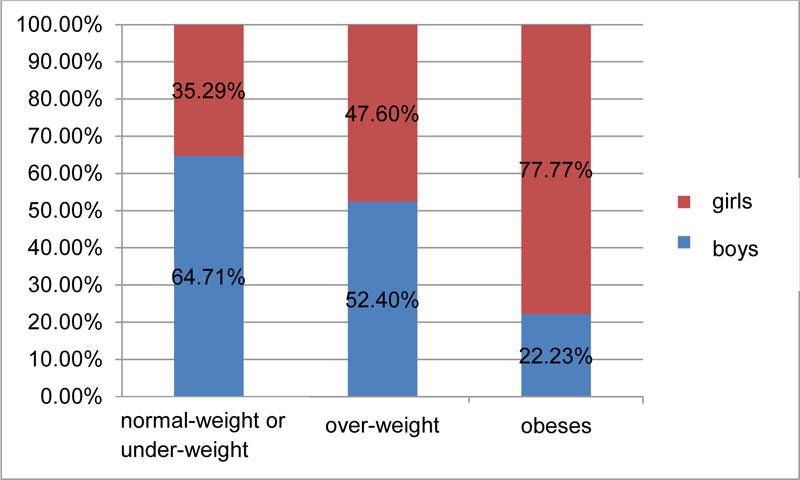
Then, we calculated the percentages of males and females for every weight group (underweight or normal weight, overweight, obese). (Fig.6)
3.3. Best Corrected Visual Acuity (Time 0)
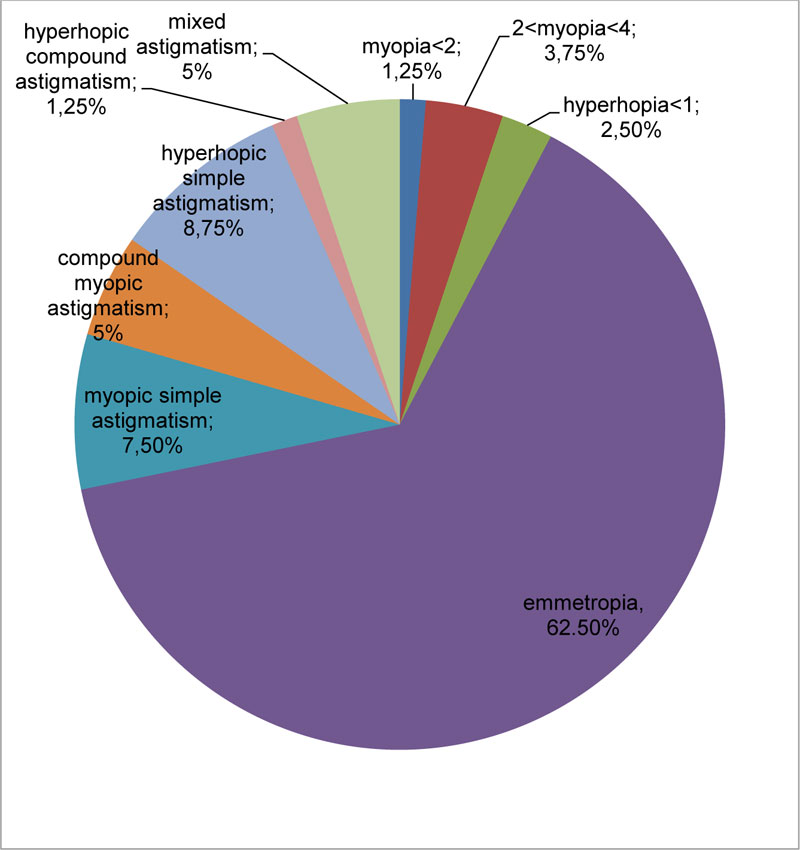
At the onset, the mean best corrected visual acuity was 8.725/10 (sd 2.264).
The refractive errors are listed in Fig. (7)
The mean myopic refractive error was 0.265 (sd 0.706), the mean subjective hyperopic refractive error was 0.043 (sd 0.195), and the mean astigmatic refractive error was 0.231 (sd 0.432).
67.5% of the patients had a best corrected visual acuity at time 0 of 10/10.
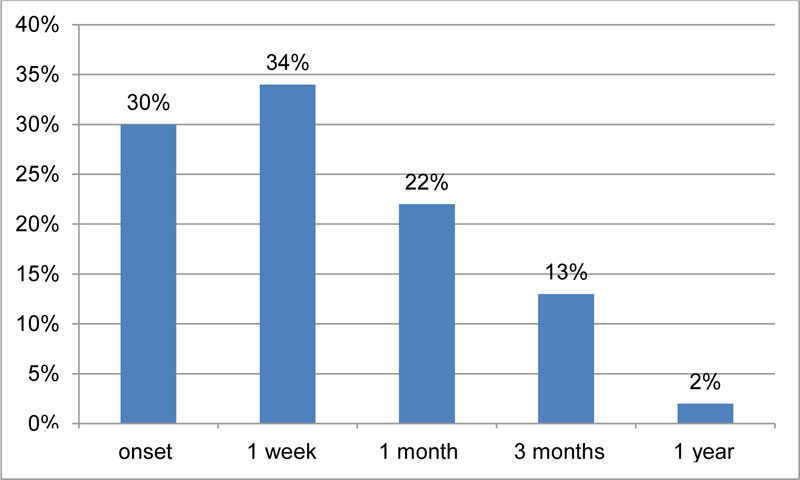
3.4. Relative Afferent Pupillary Defect
30% of our population had a relative afferent pupillary defect (RAPD) at time 0. One year after the onset, almost all patients had no longer RAPD. (Fig. 8).

3.5. VI Cranial Nerve Deficit
At the onset, 33.33% of the patients had a VI cranial nerve deficit; 1 week after the onset, the percentage increased to 37.24% and 1 month after the onset, it decreased to 14.33%. After the first month, no deficit was observed. (Fig. 9)
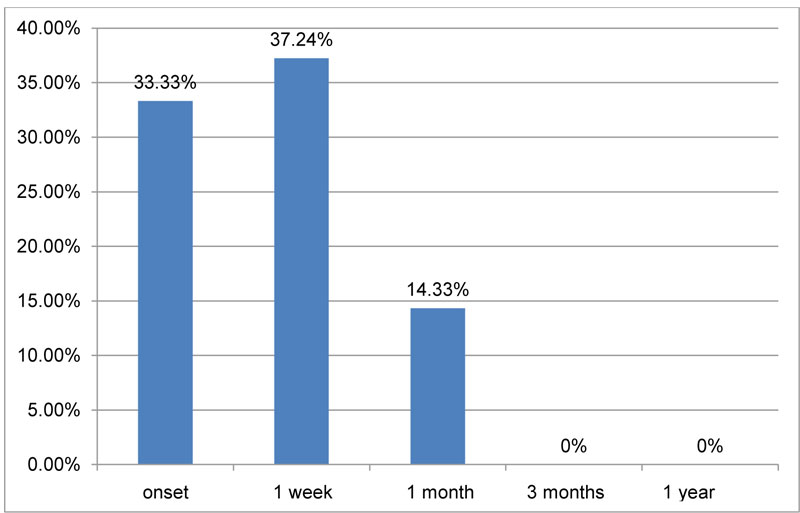
No statistically significant correlation (p) was observed between the deficit of the VI cranial nerve and Frisen classification of the severity of papilledema.
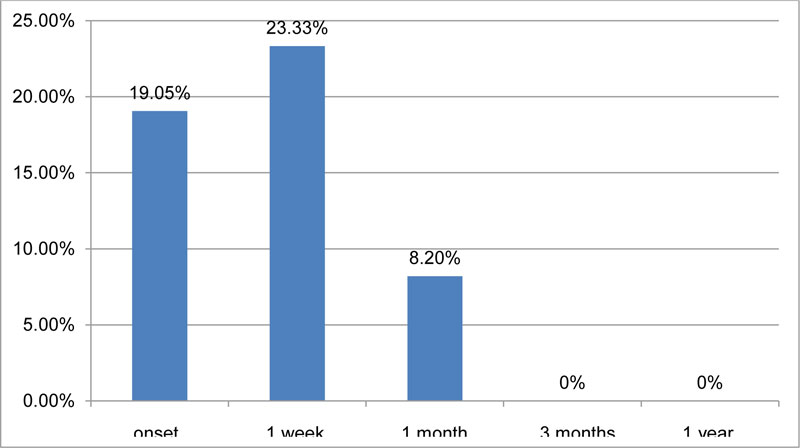
3.6. Diplopia
At the onset, 19% of the patients presented diplopia; however, after the first month, all of the patients resolved it. (Fig. 10)
Curiously, not all patients with VI cranial nerve deficit developed diplopia, as a case of bilateral VI cranial nerve deficit appeared without diplopia.
3.7. Visual Field (Time 0)
72 eyes were studied at time 0 with automated perimetry (Humprey, sita standard, 30-2); among those, 26 eyes were subjected also to manual perimetry (Goldmann) while 8 eyes were only examined with manual perimetry due to the difficulty in patient compliance (children aged 5 or less).
At time 0, the mean MD (mean defect) was -3.831 dB (sd 5.234). We evaluated only the automated Humprey perimetry.
3.8. Frisen Classification (Time 0)
The mean Frisen classification grade at the onset was 2.736 (sd 1.061) for the right eyes, and 2.631 (sd 1.213) for the left eyes.
3.9. Best Corrected Visual Acuity (Time 3)
At time 3 (1 month after the onset), the mean best corrected visual acuity was 9,132/10 (sd 3,165).
3.10. Frisen Classification (Time 3)
The mean Frisen classification grade 1 month after the onset was 2.512 (sd 1.129).
3.11. Best Corrected Visual Acuity (Time 5)
At time 3 (6 months after the onset), the mean best corrected visual acuity was 9,981/10 (sd 0.224).
3.12. Frisen Classification (Time 5)
The mean Frisen classification grade at 6 months after the onset was 0. Just 3 patients showed grade 1 bilaterally.
3.13. Diagnosis Timing
After the onset of the referred symptoms, the diagnosis was made after a mean of 17 days (sd 17.11).
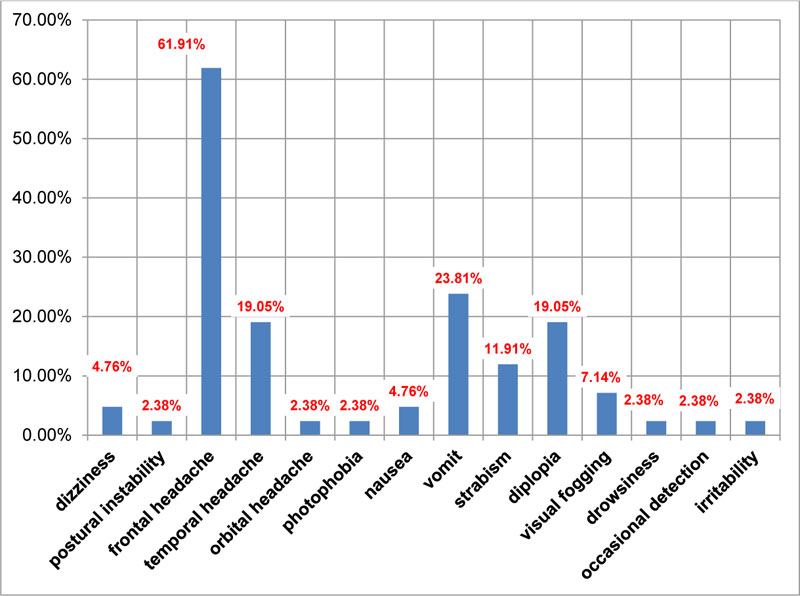
3.14. Onset Symptoms
The onset symptoms are listed in (Fig. 11).
Then, we reclassified onset symptoms per weight classes (underweight or normal weight, overweight, obese – on the basis of “BMI Z-scores CDC 2000 growth charts”). (Tables 1 and 2) (Fig. 12)
3.15. Diagnosis Delay – Best Corrected Visual Acuity / MD Correlation at Time 0
Patients with more striking (nausea, vomit, postural instability) symptoms were first diagnosed.
We did not find any statistically significant correlation (p) between diagnosis delay (days) and best corrected visual acuity or MD al the onset (p<0.005).
3.16. Diagnosis Delay – Frisen Grade at Time 0 Correlation
We calculated a statistically significant negative correlation (p -0.3) (p<0.005) between diagnosis delay (days) and Frisen classification grade at time 0.
| Weight Status Category | Percentile Range |
|---|---|
| Underweight | Less than 5th percentile |
| Normal or Healthy Weight | 5th percentile to less than 85th percentile |
| Overweight | 85th to less than 95th percentile |
| Obese | Equal to or greater than 95th percentile |
| Symptoms | Normal-weight or under-weight | Over-weight | Obese |
|---|---|---|---|
| Headache | 88,24% | 82,35% | 81,40% |
| Dizziness | 0% | 11,76% | 0% |
| Postural instability | 0% | 4,16% | 0% |
| Photophobia | 0% | 0% | 11,11% |
| Nausea | 0% | 4,16% | 11,11% |
| Vomit | 35,29% | 17,64% | 0% |
| Strabism | 11,76% | 58,82% | 22,22% |
| Diplopia | 11,70% | 47,05% | 22,22% |
| Visual fogging | 0% | 17,64% | 8,11% |
| Drowsiness | 0% | 5,88% | 0% |
| Occasional detection | 0% | 5,88% | 0% |
| Irritability | 0% | 5,88% | 0% |

3.17. Resolution Timing and Recurrence Rate
The mean resolution time was 6.56 months (sd 3.62). 3 cases (19.51%) relapsed one time within 2 year and 2 cases (4.88%) relapsed many times, the first within 3 years and the second within 5 years after the onset.
4. DISCUSSION
We observed 2 age peaks in our population, one consisting of adolescents and one consisting of younger children, aged between 4 and 7 years.
Balcer et al. [21] also observed these epidemiological features in their study, underlying a female prevalence in the adolescent group, probably related to endocrinological correlations.
Brara et al. [22] investigated the association between the risk of intracranial hypertension and overweight, mild obesity and obesity in children. They reported a strong correlation, especially in the adolescents and extremely obese Caucasian females.
Because of the close correlation with the menarche period, a hormonal role in the hypothalamic-hypophyseal-ovarian axis has been hypothesized, even if simple pre-pubertal weight gain could explain by itself the increased risk of Pseudotumor. These features indicate the similarity between the adolescent group of our studied population and the typical adult disease and its epidemiological characteristics, linked to weight gain and hormonal changes.
A correlation between Pseudotumor and estrogens, hormonal therapies, growth hormone, renal diseases, androgens and Caucasian race has been demonstrated. [17, 22-22]
We found a statistically significant correlation (p<0,005, Pearson 0,219) between age and BMI, demonstrating a stronger association between BMI and disease in older patients, in post-pubertal ages.
The classic onset symptoms were headache, nausea, vomit, blurred vision, diplopia, strabism and postural instability. [30-37]
Brara et al. [22] and Bassan et al. [38] demonstrated more symptoms in overweight/obese children, while normal weight children are often more asymptomatic.
We found only one totally asymptomatic case, during a routine visit, a 6 years old overweight Down syndrome child. In literature, Down syndrome is often correlated with occasional detection of Pseudotumor disease. [39-45]
Headache was the main onset symptom in our work; as in literature, in all weight groups, but especially in normal weight children, it was the only symptom found in 88.24% of the population, while in overweight children, we found an increased variability of symptoms.
The visual acuity did not extremely reduce, as also demonstrated in literature in case of pediatric populations. [46]
In literature, the paralysis of numerous cranial nerves, III [30, 47], IV [30, 36, 48], VI [30, 36, 48], VII [30, 36, 49], IX [47] and XII [47] has been reported. We found only the paralysis of the VII cranial nerve, in 33.33% of our population. Paley et al. [50] observed that the VII cranial nerve paralysis is common in children (8-64%), while it is infrequent in adults.
In our study, the deficit of the VI cranial nerve and the diplopia were resolved within the first month, despite the longer time of resolution of the papilledema. We did not find a correlation between the severity of papilledema and the presence of VI cranial nerve paralysis.
We found that patients with a larger optic disc could be more difficult to diagnose or they show symptoms later, by going to the medical emergency with a major delay.
However, the recurrent cases were the ones later diagnosed and we found a positive statistically significant correlation between early diagnosis and slower recovery, despite the therapy.
The relative afferent pupillary defect (RAPD) is a sign of dysfunction of the anterior optic pathways, and it is a sign of asymmetry of disease. [51] We found RAPD in 30% of the population at the onset and only in 2% after one year of disease.
28.57% of our patients at the onset had a different Frisen classification of papilledema between the two eyes, so this could explain the high percentage of RAPD at the onset compared to the literature [1]. Almost all the population resolved the RAPD within the first year of pathology, without showing any adverse consequences.
An interesting characteristic of the idiopathic intracranial hypertension is that some patients with signs of intracranial hypertension do not show papilledema [52, 53]. It seems so that some factors could predispose an optic disc to become swollen in case of intracranial hypertension. Local anatomic factors, as disc diameter or cup diameter, could be involved.
It has been demonstrated [54] that a small C/D ratio is a predisposing factor for the swollen optic disc in case of non arteritic anterior optic neuropathy.
Geddie et al. [55] and Dai et al. [56] calculated an overrepresentation of a small C/D ratio in patients with pseudotumor cerebri.
The C/D study must be related to the study of the refractive defect, because of the correlation between hyperopic defect and small C/D. [56].
In our population, almost all of the patients were emmetropic, and the refractive defect was not linked to the anatomy of the disk.
Indeed, we calculated a correlation (p 0.432) between MD and Frisen classification, confirming the perimetry as an essential factor in pseudotumor, but with a good anatomic and functional correlation for only early stages of disease.
CONCLUSION
The Pediatric Idiopathic Intracranial Hypertension or Pseudotumor Cerebri is, even nowadays, a little known pathology, both in the pediatric and ophthalmological framework.
To provide a correct diagnostic assessment, it will be essential first of all to make a correct differential diagnosis with other organic pathologies; however, in fact, Psedotumor always remains a diagnosis of exclusion.
It will be imperative to study the general and pharmacological anamnesis, reconsidering the epidemiological features of this disease.
Finally, regarding prognosis, we have found that an early detection is indispensable for the good resolution of the disease, and that pediatric cases, unlike the adult disease, often result in complete resolution without complications if handled correctly.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
It was a retrospective epidemiological desk study that does not need ethical approval.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants enrolled in the study.
AVAILABILITY OF DATA AND MATERIALS
The data generated and analyzed during this study are stored in the repository of the Department of Surgical Sciences of the University of Turin, and can be provided from the corresponding author, [FM], upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

