All published articles of this journal are available on ScienceDirect.

Assessment of Knowledge, Attitude, and Practice Regarding COVID-19 Ocular Manifestations in the Western Region of Saudi Arabia
Authors Info & Affiliations
Abstract
Introduction:
Ocular manifestations, such as conjunctivitis, redness, and tearing, were reported in patients with Coronavirus Disease 2019 (COVID-19).
Objective:
To investigate the level of knowledge, attitude, and practice about the ocular manifestations of COVID-19 and protective eye measures among the general population in the western region of Saudi Arabia.
Methods:
A cross-sectional study was conducted over two months with 800 participants from the general population and a 39-item online structured validated questionnaire using Google Forms. The collected data were analyzed using the SPSS program version 20 and a P-value <0.05 was considered statistically significant.
Results and Discussion:
Among the participants (n = 800), 71.9% were females, 50% were highly educated, and 61.8% had moderate incomes. The overall mean total knowledge score was 25.185 ± 3.774, with significant differences regarding age group, gender, and income. Most of the Saudi residents with high monthly incomes, especially females, were knowledgeable regarding the ocular manifestations of COVID-19 (25.0957 ± 3.4311). The average total knowledge, attitude, and practice score was 42.1419 ± 4.833, which was average (medium level), with significant differences regarding age group, gender, and income; a high mean was obtained from the age group >50–60, females, and high-income class.
Conclusion:
Detailed information about the epidemiology of COVID-19 and an understanding of emerging related health issues, such as ocular manifestations, should be empowered to the public while considering the least knowledgeable groups.
1. INTRODUCTION
In December 2019, an epidemic emerged from the city of Wuhan, China. The World Health Organization (WHO) declared it an outbreak of a new strain of coronavirus, which had previously not affected humans, and named it the Coronavirus Disease 2019 (COVID-19). COVID-19 is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). After first appearing in Wuhan, China, COVID-19 spread to Europe and then all over the world; subsequently, it was described as a pandemic [1].
COVID-19 is transmitted from an infected person with respiratory symptoms (such as sneezing and coughing) to other people via respiratory droplets (particle diameter >5–10 μm), direct exposure to the conjunctiva of the eye, and contact with contaminated surfaces. Further, some scientific studies suggested the possibility of fecal-oral transmission [2], as shown in the 2003 SARS-CoV outbreak. It was reported that SARS-CoV could be transmitted through the sewage system, especially in the absence of adequate disinfection [3]. The virus can cause a wide range of symptoms that range from mild illness to severe pneumonia, with more severe symptoms in immunocompromised patients and those with cardiopulmonary diseases. Some of these symptoms include rhinitis, fever, cough, headache, dyspnea, loss of smell (anosmia), taste disturbance, and sore throat. Patients may complain about these symptoms before testing positive for COVID-19 [4]. Some reports have implied that anosmia is the only clinical presenting symptom [5].
Many scientific studies had reported extra-pulmonary manifestations, such as conjunctival congestion and other ocular symptoms. Wu et al. [6] conducted a series of case studies, including 38 patients of COVID-19 in the Hubei province in China. The studies concluded that 12 (31.6%) patients presented with ocular manifestations, such as chemosis, epiphora, and conjunctival congestion. Among these patients, there were two patients who yielded positive real-time reverse transcription-polymerase chain reaction (RT-PCR) tests from their conjunctival swabs. A recent study in China by Chen et al. [7] reported ocular manifestations in 534 patients of COVID-19 in two investigated hospitals. These patients had symptoms that included conjunctival congestion, foreign body sensation, increased secretion, and eye dryness. Three of these patients had conjunctival congestion as an initial symptom of COVID-19 simultaneously with positive PCR nasopharyngeal swabs. As conjunctival congestion is a common presenting symptom of COVID-19, an ophthalmologist may be needed to consult in COVID-19 cases [8]. Due to a lack of epidemiologic research about COVID-19, there is no current specific treatment or vaccine but only supportive management of the clinical symptoms, such as cough, fever, and sneezing. However, the similarity between SARS-CoV-2 and SARS-CoV may enable health workers to use the same therapeutic management used with SARS-CoV in the future [9].
Improving public awareness about COVID-19 is necessary in order to eliminate the spread of the disease, including the implementation of new strategies and preventive measures, such as strict personal hygiene (washing hands for at least 20 seconds and avoiding touching the eyes, face, and mouth), wearing face masks, isolating infected cases, social and physical distancing, and ensuring that people who are immunocompromised avoid public places [10]. Other preventive strategies should be applied in case of healthcare workers, especially those who care for patients of COVID-19-, such as precautions regarding airborne transmission by including the use of Personal Protective Equipment, (PPE) consisting of N95 or FFP3 (face-fit respiratory masks) masks, eye protection, gowns, and gloves to reduce the transmission of the pathogen [11].
Many strategies have been implemented at national levels to raise public awareness about the manifestations of COVID-19, including ocular strategies through informative mobile messages, awareness posters, and TV shows to maintain a high level of personal hygiene and protective measures [12].
2. MATERIALS AND METHODS
2.1. Type of Study
This study was an observational cross-sectional study that aimed to investigate the level of Knowledge, Attitude, and Practice (KAP) about the ocular manifestations of COVID-19 and eye protection measures among the general population in the western region of Saudi Arabia. The study was conducted over a two-month period from April–May, 2020.
Each participant was informed about the aim of the study and gave informed consent. People who did not consent were unable to participate, or did not submit completed questionnaires were excluded from the study.
2.2. Data Collection
A semi-designed online questionnaire, obtained from Labban et al. [13], was uploaded on Google Forms. The final form was reviewed for its validation and reliability by more than one expert via a back-translation technique wherein the questionnaire was translated twice to Arabic and then back to English to prevent a language barrier. The two translated copies were compared to ensure that they conveyed the same meaning. A pilot study was first conducted with 10% of the calculated participants and was not included in this study. Cronbach's alpha was used to measure the validation; reliability of a coefficient of 0.714 was considered acceptable. This electronic questionnaire was distributed through social media websites and filters applied for the population of the western region because this was where the authors lived.
The applied questionnaire had three sections. The first section included socio-demographic data (age, gender, marital status, level of education, income, occupation, special habits, and crowding index, which was measured by dividing the number of persons in a home by the number of rooms in the home), data about medical history (chronic disease, previous exposure to COVID-19, contact with infected persons, previous ocular operations, ocular disease, and use of contact lenses).
The second and third sections of the questionnaire included questions that measured KAP to assess awareness about the epidemiological data of COVID-19 regarding ocular manifestations and safety measures to reduce infectivity. Seventeen questions were related to knowledge, and were scored as follows: the correct answer was given two points, I don't know” was given one point, and “No” was given zero points. Seven questions were used to assess attitude and practice. The Likert scale was applied to assess the scores, which ranged from one to three, with a total score of 55 points for all questions: 34 points for knowledge and 21 points for attitude and practice. The points were added for the answered questions. The participants who received a KAP score >50, 25–50, and <25 were considered to have performed on a high, medium, and low level, respectively.
2.3. Data Management
All data were analyzed and coded by the Statistical Package for Social Science (version 20, SPSS Inc., Chicago, IL). In the case of quantitative (continuous) normally distributed variables, the student’s t-test and analysis of variance (ANOVA) were utilized to compare the means, and a P-value <0.05 was considered to be statistically significant. The sample size was calculated using EPI INFO (Epidemiological Information Package) version (21) 3.5.3 statistical packages at a confidence interval of 95% and power of 80%.
2.4. Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Ethical Review Committee of the King Abdulaziz University Hospital. Confidentiality of data was ensured, and data was accessed only by the researchers. Consent was taken electronically as part of the survey
3. RESULTS
One thousand and one hundred electronic questionnaire links were sent, and 800 participants’ responses were included in the study after filtering and cleaning the datawith a response rate of 73%. Table 1 shows that most of the study participants were women (71.9). The age of the participants ranged from 17 to 62 years. We classified the participants into five groups: <18 (2.4%), 18–30 (57.5%), >30–40 (19%), >40–50 (14.4%), >50–60 (5.9%), and >60 (0.9%).
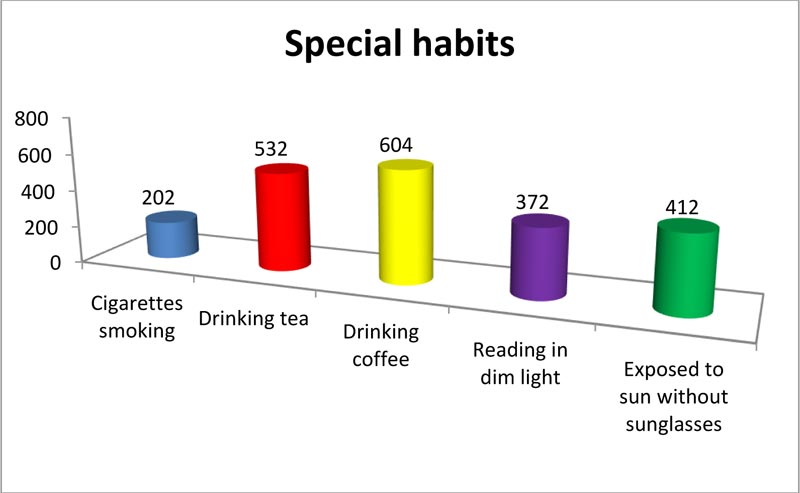
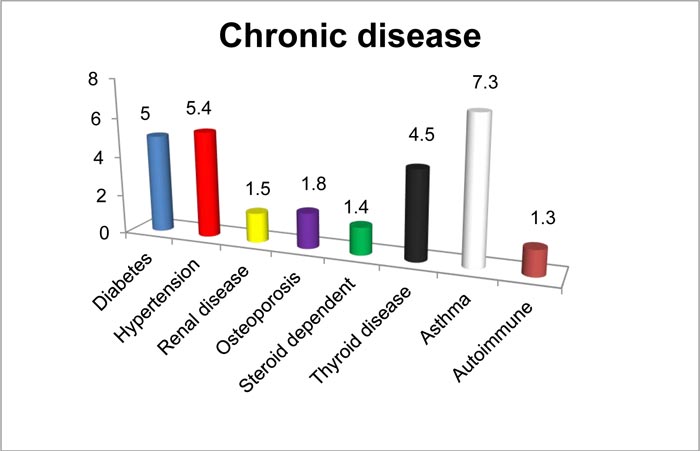
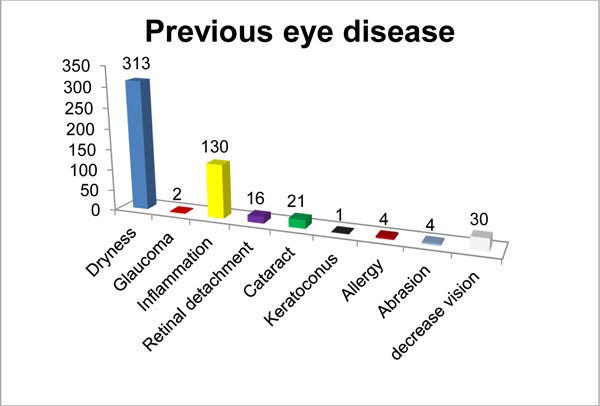
Since monthly income is one of the most important variables in the level of knowledge and practice, most of the participants (61.8%) earned moderate-income, and half of the participants were highly educated. Regarding marital status, approximately 52.9%, 42.6%, 2.8%, 1.8% of the participants were single, married, divorced, and widowed, respectively. Special habits of the respondents are demonstrated in Fig. (1) 1: 75.5% of the participants drank coffee, 25.3% of the participants smoked cigarettes, and 46.5% of the participants reported reading in dim light. The medical history (chronic disease and previous eye disease) of the participants is illustrated in Figs. (2–4).
Table 2 shows that only 3.5% of the participants were previously infected with COVID-19, 12.6% of the participants had come into contact with an infected person, 13.9% of the participants had previous eye operations, and 39.5% of the participants wore contact lenses (47.46% of contact lens wearers wore the contact lenses for medical reasons).
| Basic characteristics | Study group | |
|---|---|---|
| No. (800) | % (100) | |
|
Gender Female Male |
575 225 |
71.9% 28.1% |
|
Age group <18 18–30 >30–40 >40–50 >50–60 >60 |
19 460 152 115 47 7 |
2.4% 57.5% 19% 14.4% 5.9% 0.9% |
|
Marital status Single Married Divorced Widowed |
423 341 22 14 |
52.9% 42.6% 2.8% 1.8% |
|
Level of education Illiterate Primary school Middle school High school Higher education |
1 15 127 257 400 |
0.1% 1.9% 15.9% 32.12% 50% |
|
Income Low/Not enough Moderate/Enough High/Enough and exceed |
207 494 99 |
25.9% 61.8% 12.4% |
|
Occupation Health service provider Student in medical college Student in non-medical college Government or private employ Unemployed |
110 170 122 238 160 |
13.8% 21.2% 15.3% 29.8% 20% |
| Crowding index (X ± SD) | 5.8255 ± 2.13 | |
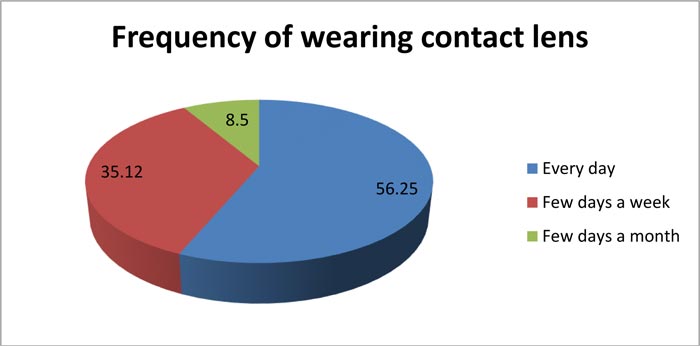
Table 3 lists the awareness and knowledge of the participants regarding COVID-19. The majority of the participants (91.9%, 95%, 87.3%, and 97%) believed that COVID-19 was caused by a virus that is transmitted from the droplets of an infected person spread by coughing and sneezing, but only 30.5% of the participants believed that the virus could be transmitted by eye tears. Only 19.5% of the participants believed that COVID-19 could show ocular manifestations; however, 61.6% of the participants believed that these manifestations could be prevented by wearing a mask, thus decreasing its incidence. The percentage of participants who considered that there was no need for an ophthalmologist to examine a patient with COVID-19 was 47.6%. Regarding correct answers, the average total knowledge score was 25.185± 3.774. There was a statistically significant difference between age groups, with a high mean value for the age group >50–60 followed by the age group >40–50. There was also a statistically significant difference regarding gender. Participants with high incomes showed more awareness than other groups.
| Study group | ||
|---|---|---|
|
No. (Total n = 800) |
% (100) | |
| Previous infection with COVID-19 | 28 | 3.5 |
| Previous contact with an infected person | 101 | 12.6 |
| Previous eye disease | 500 | 62.5 |
| Previous eye operation | 111 | 13.9 |
| Using eye drops | 119 | 14.9 |
|
Wearing contact lenses (For medical reasons) |
316 (150) |
39.5 (47.46) |
| Items related to knowledge |
No. (n = 800) |
% (100) | |
|---|---|---|---|
| COVID 19 is caused by a virus | Yes No I don't know |
735 10 55 |
91.9 1.3 6.9 |
| COVID 19 is transmitted by infected persons through droplets | Yes No I don't know |
760 17 23 |
95 2.1 2.9 |
| COVID 19 is transmitted by droplets on surfaces | Yes No I don't know |
698 38 64 |
87.3 4.8 8.0 |
| COVID 19 is transmitted by coughing and sneezing | Yes No I don't know |
776 4 20 |
97 0.5 25 |
| COVID 19 is transmitted by eye tears | Yes No I don't know |
244 176 380 |
30.5 22 47.5 |
| COVID 19 has upper respiratory and lower respiratory symptoms | Yes No I don't know |
768 8 24 |
96 1.0 3.0 |
| COVID 19 has ocular manifestations, such as eye redness, dryness, pain, increased secretions, feeling of foreign body sensation, and itching | Yes No I don't know |
156 65 579 |
19.5 8.1 72.4 |
| Ocular manifestation may be the only presenting symptom in COVID-19 | Yes No I don't know |
100 226 474 |
12.5 28.3 59.3 |
| COVID-19 may lead to blindness | Yes No I don't know |
29 376 395 |
3.6 47 49.4 |
| COVID-19 symptoms include gastrointestinal symptoms | Yes No I don't know |
535 50 215 |
66.9 6.3 26.9 |
| COVID 19 symptoms include fever and muscle pain | Yes No I don't know |
765 6 29 |
95.6 0.8 3.6 |
| Washing hands for 20 seconds can protect the eye and decrease the incidence of eye manifestations | Yes No I don't know |
654 52 94 |
81.8 6.5 11.8 |
| COVID-19 ocular manifestations can be prevented by wearing a mask and eyeglasses | Yes No I don't know |
493 84 223 |
61.6 10.5 27.9 |
| COVID-19 can be prevented by having a strong immune system | Yes No I don't know |
582 112 106 |
72.8 14 13.3 |
| COVID-19 requires examination by an ophthalmologist | Yes No I don't know |
134 285 381 |
16.8 35.6 47.6 |
| Wearing contact lenses increases the incidence of COVID-19 infection | Yes No I don't know |
217 134 449 |
27.1 16.8 56.1 |
| Wearing eyeglasses is better than contact lenses to decrease infection | Yes No I don't know |
313 88 399 |
39.1 11 49.9 |
| Total score; mean ± SD (>median) | 25.185 ± 3.774 (median = 25) | ||
| Items related to attitude and practice |
No (n = 800) |
% (100) | |
|---|---|---|---|
| Wash hands before and after wearing contact lens (total n = 316) | Always/most of the time Sometimes/occasionally Rarely |
208 40 68 |
65.82 12.65 21.5 |
| Wear protective measures, such as masks | Always/most of the time Some-time/occasionally Rarely |
724 63 13 |
90.5 7.9 1.6 |
| Share eye cosmetic products (total n = 575) | Always/most of the time Sometimes/occasionally NA (225) |
339 236 |
58.95 41.04 |
| Response to quarantine regulations | Always/most of the time Sometimes/occasionally Rarely |
741 47 12 |
97 5.9 1.5 |
| Consulting ophthalmologist during quarantine in case of eye problem | Always/most of the time Sometimes/occasionally Rarely |
286 237 277 |
35.7 29.6 34.7 |
| Going to hospital during quarantine in case of eye problem | Always/most of the time Sometimes/occasionally Rarely |
354 237 209 |
44.2 29.7 26.1 |
| Total score; mean ± SD (>median) | 17.1622 ± 2.658 (median = 17) | ||
| Items | Total knowledge score (mean ± SD) | Total attitude and practice score (mean ± SD) | Total score (mean ± SD) |
|---|---|---|---|
|
Age <18 18–30 >30–40 >40–50 >50–60 >60 P-value |
22.894 ± 2.579 24.3739 ± 3.8188 24.9079 ±3.8487 25.7739 ± 3.311 26.8085 ± 3.468 24.4286 ± 3.5523 0.04** |
17 ± 2.08 16.589 ± 2.695 16.794 ± 2.703 16.8609 ± 2.618 17.7872 ± 2.254 18.2857 ± 2.360 0.04* |
39.8947 ± 3.914 40.963 ± 4.862 41.6755 ± 4.711 42.6348 ± 4.548 44.5957 ± 4.384 42.7143 ± 4.923 0.02** |
|
Gender Male Female P-value |
23.9911 ± 4.446 25.0957 ± 3.4311 0.001* |
16.3661 ± 3.006 16.9165 ± 2.4959 0.08 |
40.3348 ± 5.550 42.0 ± 4.440 0.03** |
|
Income Low/Not enough Moderate/Enough High/Enough and exceed P-value |
23.859 ± 3.961 24.931 ±3.67 25.989 ± 3.462 0.02** |
16.57 ± 2.662 16.685 ± 2.6273 1a7.545 ± 2.696 0.02** |
40.43 ± 4.752 41.6085 ± 4.797 43.535 ± 4.529 0.04** |
Regarding the attitude and practice toward eye protection during the COVID-19 pandemic, including washing hands before and after wearing eye lenses, wearing protective masks, and not sharing cosmetic eye products, the results were 66%, 90.5%, and 42.4%, respectively. A total of 34.7% had no idea that it is important to consult ophthalmologists, with a total attitude and practice score of 17.162 ± 2.658, which is considered above the median and good attitude. There were statistically significant differences among different age groups and income levels (Tables 4 and 5), respectively, but no significant difference was obtained regarding gender.
By measuring the correct answers among the participants, the total average KAP score was 42.1419 ± 4.833, which was considered to be average (medium level), with a significant difference among different age groups, gender, and income levels (Table 5).
4. DISCUSSION
Globally, COVID19 showed rapid spread that forced all countries into states of emergency [14]. This study is a cross-sectional study that was conducted to investigate the level of KAP about COVID-19 ocular manifestations and protective measures regarding eyes. It included 800 participants in the western region of Saudi Arabia. There was a higher rate of female respondents towards the survey. [15]. In this study, 95% of the studied participants believed that COVID-19 was transmitted from the droplets of an infected person, and 97% of participants believed that it was transmitted via coughing and sneezing that may reach the eye. This was in concordance with a study done in China (Hubei province), which showed that wearing eyeglasses for more than 8 hours a day may protect the general population from COVID-19 [16]. However, this study had many limitations, as it was done during the early stages of the pandemic and it did not include hand washing and social distancing as protective measures. The health guidelines recommended that mainly health care professionals wear PPE, such as face-shield with face masks in order to protect their eyes from viral spread through respiratory droplets [17].
About their general knowledge concerning COVID-19, the majority of the participants (96%) reported that it presented with upper and lower respiratory manifestations, while 59.3% had no idea about the ocular manifestations of the virus. However, Pandey et al. [18] performed a survey of more than 745 subjects from the Indian population to assess their awareness about COVID-19, and nearly 42.9% believed that respiratory illness, cough, and fever were symptoms of COVID-19. The study also found that a considerable number of participants were not aware that ocular manifestations could be caused by the virus. Rothe et al. [19] detected ocular manifestation, such as conjunctivitis that can be found at the onset of COVID-19 in many patients.
In this study, 3.6% of the participants believed that COVID-19 could lead to blindness, as described in a case report wherein a patient admitted to a hospital with a 5-day history of fever and a positive PCR (RT-PCR) test for SARS-CoV-2 suddenly developed vision loss in both eyes and could only recognize waving hands. It was suggested that SARS-CoV-2 could lead to brain tissue edema and partial neurological degeneration like other viruses. However, there is no solid evidence for this explanation [20].
Al-Hanawi et al. [21] discovered that a high knowledge score presented in older adults, which corresponded to our study results since the age group >50–60 had better knowledge, followed by the age group >40–50. Akalu et al. [22] reported high monthly income was associated with a 20% decrease (Odds Ratio [OR] = 0.8) in the likelihood of having poor knowledge. Low income may lead to powerlessness to change one's conduct or condition, leading to failure to execute suggested defensive measures against COVID-19 [23].
Measuring the attitude and practice among the studied participants showed optimistic attitudes and good practices toward COVID-19 regarding washing hands before and after wearing contact lens, wearing protective measures, such as face masks, not sharing cosmetic eye products, and consulting ophthalmologists in case of any eye problem based on the idea that COVID-19 is capable of causing some ocular symptoms and may lead to complications. These results are better than what was reported by Akalu et al. [22]. The Center for Disease Control (CDC) recommended general guidelines indicating that extra care should be taken by those wearing contact lenses through the use of sterile containers and washing lenses with saline; however, they do not prefer it at all [24]. As protection is better than treatment, we tried to help the general population enact safe practices in this pandemic situation.
4.1. LIMITATIONS
One of the limitations of this study was that it depended on self-reported online questionnaires. Attitude and practice are better assessed using focus groups or in-depth interviews. However, this was not applicable in our study due to factors such as time limitations and the current pandemic.
CONCLUSION
Detailed information about the epidemiology of COVID-19 and an understanding of emerging related health issues, such as ocular manifestations, should be empowered to the public, keeping in mind the least knowledgeable groups.
LIST OF ABBREVIATIONS
| WHO | = World Health Organization |
| CDC | = Center for Disease Control |
| COVID-19 | = Coronavirus Disease 2019 |
| SARS-CoV-2 | = Severe Acute Respiratory Syndrome Coronavirus 2 |
| RT-PCR | = Reverse Transcription-Polymerase Chain Reaction |
| PPE | = Personal Protective Equipment |
| KAP | = Knowledge, Attitude, and Practice |
| ANOVA | = Analysis of Variance |
| OR | = Odds Ratio |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Research Ethics Committe of King Abdulaziz University Hospital, Saudi Arabia under approval number 556-20.
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written consent was taken from all the study participants.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author, [M.A] upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

