All published articles of this journal are available on ScienceDirect.

The Prevalence and Risk Factors for Symptomatic Dry Eye in Adults in Riyadh, Saudi Arabia
Authors Info & Affiliations
Abstract
Objectives:
The objective of this study is to estimate the prevalence of symptomatic suspected dry eye, diagnosed dry eye syndrome (DES), and associated risk factors; in Riyadh, Saudi Arabia.
Methods:
A cross-sectional study of 654 participants was employed using a self-administered semi-structured questionnaire that included demographic characteristics like age, gender, and risk factors (smoking, using contact lenses, chronic comorbidities, etc.).
Results:
There were 266 (40.7%) previously diagnosed DES participants and 388 (59.3%) non-diagnosed DES, of which 497 were female and 157 were male. Females had a significantly higher rate of diagnosed DES than males (p<0.001), with a significant increase in the rate of DES diagnosis with age (p<0.001). There was also a significant increase in DES in participants with diabetes mellitus, allergic eye, thyroid eye, and skin diseases, as well as having undergone laser surgery or using contact lenses. There was no significant increase in DES in cases of smoking, daily use of electronic devices, or duration of sleep.
Conclusion:
The prevalence of dry eye among adults in Riyadh was 46.6%, with the most important risk factors being female gender, increasing age, Lasik refractive surgery, skin disease around the eye, and thyroid eye disease.
1. INTRODUCTION
Dry eye syndrome (DES) is a common chronic disease of the ocular surface [1, 2]. The primary components of tears are mucin, aqueous, and lipid layers, which combine to create a complex viscoelastic structure. The lacrimal and accessory lacrimal glands produce the aqueous layer, the goblet cells of the conjunctiva produce the mucin layer, and the meibomian glands produce the lipid layer. This complex structure is responsible for lubrication nutrition as well as protecting the cornea. The lipid layer prevents evaporation and stabilizes tears Deficiency of any of the three layers may lead to symptoms of DES [3].
DES has significant socio-economic implications, such as increased healthcare costs and a negative impact on vision-related quality of life issues, such as driving, television watching, reading, computer work, and emotional wellbeing [4]. The validated six-item questionnaire of ocular symptoms related to dry eye [5, 6] is a widely used effective tool to assess the presence of dry eye; nonetheless, the prevalence of DES is difficult to assess due to the variability and inconsistency of symptoms, methods of diagnosis, and a poor link between symptoms and signs frequently encountered in other eye conditions [7]. Consequently, the prevalence may be underestimated [8-10], varying widely between studies, regions, and countries. However, despite the high prevalence of DES, no cure is available; therefore, early recognition and prevention are important to improve patients' symptoms with primary preventive measures such as education and elimination of risk factors.
This study aimed to estimate the prevalence of diagnosed and symptomatic suspected DES and its relation to risk factors in adults in Riyadh, Saudi Arabia.
2. MATERIALS AND METHODS
This cross-sectional study of Saudi adults (>18 years) in Riyadh, Saudi Arabia used a self-administered semi-structured questionnaire designed to cover the symptoms and signs of dry eye. This study was conducted from November 2019 to March 2020 and included 654 participants. Participants were included in the study provided they completed all components of the questionnaire, which included informed consent. The questionnaire included demographic characteristics like age and gender, as well as risk factors (smoking, using contact lenses, chronic comorbidities, etc.). In addition, the questionnaire included multiple lifestyle factors that were hypothesized to be associated with DES.
A validated six-item questionnaire of ocular symptoms related to the dry eye has been used for the assessment of DES [5, 6]. This questionnaire was developed as a patient-centered self-assessment to assist healthcare providers in diagnosing DES and assessing the symptoms of the syndrome, feeling sandy sensation, burning eyes, red eyes, crusting on lashes, stuck eyes, and feeling dry or uncomfortable with air conditioning. The frequency of a symptom was scored as never, rarely (at least once in 3-4 months), sometimes (once in 2-4 weeks), often (at least once a week), or constantly (all the time).
2.1. Ethical Considerations
Participants provided informed consent. Confidentiality of the responses was maintained strictly to ensure the privacy of their data and protect their anonymity. The participants had the right to withdraw from the study at any time. The study adhered to the guidelines of the Declaration of Helsinki.
2.2. Data Analysis
A participant was considered positive if they were previously diagnosed as DES and complained of at least one symptom of DES sometimes, often, or constantly, or if they were previously undiagnosed DES but complained of at least one symptom of DES often or constantly. Data were expressed as numbers and percentages, and statistical analyses were performed using the Statistical Package for the Social Sciences software, version 19.0 (SPSS Inc, Chicago, IL, USA). The chi-square test was used to compare groups.
3. RESULTS
A total of 654 questionnaires were completed in this study. There were 497 female respondents and 157 male respondents, of which 266 (40.7%) were previously diagnosed as DES and 388 (59.3%) were not diagnosed as DES. The demographic and clinical data of the participants are shown in Table (1). Females had a significantly higher rate of diagnosed DES than male participants (p<0.001), with a significant increase in the rate of diagnosis of DES with age (p<0.001). There was also a significant increase in DES in those participants with allergic or thyroid eye disease, diabetes mellitus, and skin diseases or those having undergone laser surgery or using contact lenses, whereas smoking, daily use of electronic devices, or sleeping duration had no impact on DES diagnosis (Table 1).
| Characteristics | Non-Diagnosed DES, n (%) | Diagnosed DES, n (%) | P-value* |
|---|---|---|---|
| Gender | |||
| Female, n = 498 (76.15%) | 275 (70.88%) | 223 (83.83%) | |
| Male, n = 156 (23.85%) | 113 (29.12%) | 43 (16.17%) | <0.001 |
| Age | |||
| 18 to 29 yrs, n = 158 (24.16%) | 116 (29.90%) | 42 (15.79%) | |
| 30 to 40 yrs, n = 154 (23.55%) | 91 (23.45%) | 63 (23.68%) | |
| >40 yrs, n = 342 (52.29%) | 181 (46.65%) | 161 (60.53%) | <0.001 |
| Allergic eye disease | |||
| No, n = 486 (74.31%) | 325 (83.76%) | 161 (60.53%) | |
| Yes, n = 168 (25.69%) | 63 (16.24%) | 105 (39.47%) | <0.001 |
| Lasik surgery | |||
| No, n = 504 (77.06%) | 315 (81.19%) | 189 (71.05%) | |
| Yes, n = 150 (22.94%) | 73 (18.81%) | 77 (28.95%) | 0.002 |
| Using contact lenses | |||
| No, n = 544 (83.18%) | 332 (85.57%) | 212 (79.70%) | |
| Yes, n = 110 (16.82%) | 56 (14.43%) | 54 (20.30%) | 0.048 |
| Using electronic devices | |||
| <2 hrs, n = 49 (7.49%) | 31 (7.99%) | 18 (6.77%) | |
| 2-4 hrs, n = 260 (39.76%) | 148 (38.14%) | 112 (42.11%) | |
| 5-7 hrs, n = 228 (34.86%) | 137 (35.31%) | 91 (34.21%) | |
| >7 hrs, n = 117 (17.89%) | 72 (18.56%) | 45 (16.92%) | 0.746 |
| Sleeping hours | |||
| 5-7 hrs, n = 496 (75.84%) | 284 (73.20%) | 212 (79.70%) | |
| 8-10 hrs, n = 158 (24.16%) | 104 (26.80%) | 54 (20.30%) | 0.056 |
| Skin disease | |||
| No, n = 589 (90.06%) | 369 (95.10%) | 220 (82.71%) | |
| Yes, n = 65 (9.94%) | 19 (4.90%) | 46 (17.29%) | <0.001 |
| Diabetes Mellitus | |||
| No, n = 566 (86.54%) | 346 (89.17%) | 220 (38.87%) | |
| Yes, n = 88 (13.4%) | 42 (10.82%) | 46 (52.27%) | 0.017 |
| Thyroid disease | |||
| No, n = 566 (86.54%) | 348 (61.48%) | 218 (81.95%) | |
| Yes, n = 88 (13.46%) | 40 (45.45%) | 48 (18.05%) | 0.004 |
| Smoking | |||
| No, n = 621 (94.95%) | 365 (94.07%) | 256 (96.24%) | |
| Yes, n = 33 (5.05%) | 23 (5.93%) | 10 (3.76%) | 0.213 |
* χ2
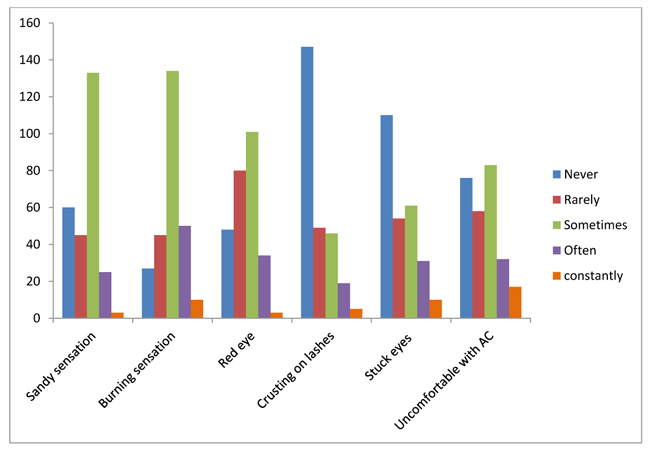
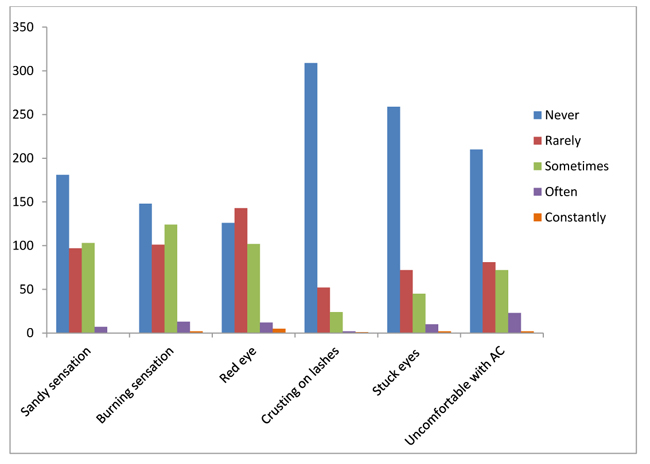
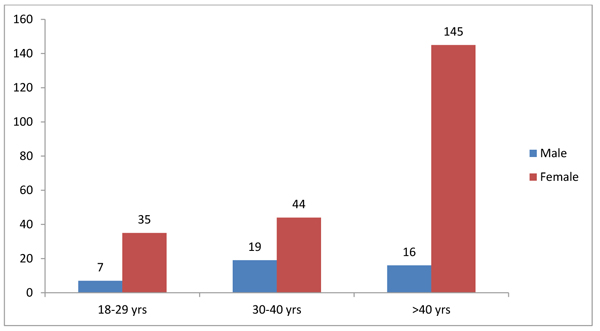
In diagnosed DES, 116 participants (43.6%) reported experiencing one or more symptoms often or constantly: one symptom in 51 participants (19.2%), two symptoms in 30 participants (11.3%), three symptoms in 21 participants (7.9%), four symptoms in 7 participants (2.6%), five symptoms in 6 participants (2.6%), and 6 symptoms (all symptoms) in 1 participant (0.4%). The symptoms reported included burning sensation (60 participants; 22.6%), feeling uncomfortable with AC (59 participants; 22.2%), stuck eyes (41 participants; 15.1%), red eyes (37 participants; 13.9%), sandy sensation (28 participants; 10.5%), and crusting on the eyelashes (24 participants; 9.0%) (Table 2). The distribution of symptoms of dry eye in participants diagnosed with DES is illustrated in Fig. (1). In previously non-diagnosed DES, 56 participants (14.4%) reported experiencing one or more symptoms often or constantly (Table 3), with an overall 172/654 (26.3%). The distribution of dry eye symptoms in participants non-diagnosed as DES is illustrated in Fig. (2). The age and sex distribution among diagnosed DES are shown in Fig. (3). The most infrequent symptoms reported as often or constantly were crusting on eyelashes and stuck eyes in the morning. Seventeen participants of the previously diagnosed DES group reported symptoms as never or rare only; hence, they were considered negative participants for DES, and the remaining 249 were considered positive for DES. Fifty-six participants of the previously non-diagnosed DES group reported one or more symptoms as often or constantly and were considered positive for DES; hence there were 305/654 (46.64%) positive participants.
| - | Never | Rare | Sometimes | Often | Constantly |
|---|---|---|---|---|---|
| Sandy sensation | 60 (22.56%) | 45 (16.92%) | 133 (%) | 25 (%) | 3 (%) |
| Burning sensation | 27 (10.15%) | 45 (16.92%) | 134 (50.38%) | 50 (18.80%) | 10 (3.76%) |
| Red eye | 48 (18.05%) | 80 (30.08%) | 101 (37.97%) | 34 (12.78%) | 3 (1.13%) |
| Crusting on eye lashes | 147 (55.26%) | 49 (18.42%) | 46 (17.29%) | 19 (7.14%) | 5 (1.88%) |
| Stuck eyes in the morning | 110 (41.35%) | 54 (20.30%) | 61 (22.93%) | 31 (11.65%) | 10 (3.77%) |
| Feeling uncomfortable with AC | 76 (28.57%) | 58 (21.80%) | 83 (31.20%) | 32 (12.03%) | 17 (6.39%) |
| - | Never | Rare | Sometimes | Often | Constantly |
|---|---|---|---|---|---|
| Sandy sensation | 181 (46.65) | 97 (25.00%) | 103 (26.55%) | 7 (1.80%) | 0 (0.00%) |
| Burning sensation | 148 (38.14%) | 101 (26.03%) | 124 (31.96%) | 13 (3.36%) | 2 (0.52%) |
| Red eye | 126 (32.47%) | 143 (36.86%) | 102 (26.29%) | 12 (3.09%) | 5 (1.29%) |
| Crusting on eye lashes | 309 (79.64%) | 52 (13.40%) | 24 (6.19%) | 2 (0.52%) | 1 (0.26%) |
| Stuck eyes in the morning | 259 (66.75%) | 72 (18.56%) | 45 (11.60%) | 10 (2.58%) | 2 (0.52%) |
| Feeling uncomfortable with AC | 210 (54.12%) | 81 (20.88%) | 72 (18.56%) | 23 (5.93%) | 2 (0.52%) |
4. DISCUSSION
DES is an ocular surface disorder and represents one of the most common eye diseases [11]. It is a public health concern that causes significant health problems affecting visual function and quality of life. A key factor in the diagnosis of DES is identifying the risk factors and looking at the accurate and detailed medical history. DES is not associated with specific symptoms, and the symptoms may vary between individuals in terms of their type and severity. Furthermore, there may be no symptoms during the early stages of the disease. The prevalence of DES ranges from 6.8% to 87.5% [11-13].
In this study, there were 40.7% previously diagnosed DES participants, of whom 17 participants reported that they experienced symptoms never or rarely and were considered negative, indicating that the actual prevalence should depend on patient examination and tests for the dry eye rather than a self-reported questionnaire. Many participants (56 out of 388) with non-diagnosed DES having one or more symptoms of the dry eye constantly or often were suspected of having DES and considered positive for DES, thereby increasing the prevalence of DES. Consequently, the prevalence of DES in Riyadh is about 47%, one of the highest reported and may be related to the hot, dry climate in Riyadh, with residents frequently using air conditioners and fans at home and in cars. Factors affecting the variation in the prevalence of DES between studies may include the criteria of DES diagnosis, the climate, humidity, prevalence of trachoma, as well as the use of fans and air conditioners. A study conducted in AlHasa KSA in which DES was diagnosed based on the participants complaining of one or more symptoms of DES as often or constantly reported a prevalence of 32.1% (597 out of 1858) [14]. Similarly, in our study, the prevalence of participants complaining of one or more symptoms was 26.3%.
There was a significantly higher prevalence of dry eye in females than males, and this sex difference was consistent across all the age groups in the present study. This may be due to female sex hormones and their effect on the ocular surface and tear secretion, in line with other studies [12, 15-20]. Nonetheless, the sex difference consistent across all studied age groups, was not universal in previous studies [21-25].
Furthermore, aging was found to be a significant risk factor for DES as in other studies [15, 16, 18-20], possibly due to decreased tear secretion and blinking reflex that leads to increased evaporation of tears with increasing age. Also, participants with diabetes mellitus, skin disease around the eye, thyroid problems, and blepharitis were more prone to symptoms of dry eye.
5. LIMITATIONS
There are some limitations to this study; for instance, the diagnosis of dry eye was dependent on history and symptoms and signs, but no tests for DES were performed due to the COVID-19 pandemic. Also, the sample number for some items was too low for statistical analysis, e.g., smoking.
CONCLUSION
The prevalence of DES in Riyadh was 46.6%, with women being more susceptible to DES than men. Various factors were associated with an increased risk of DES, such as wearing contact lenses or having a history of vision corrected by Lasik, prolonged use of electronic devices, eye or surrounding skin allergy, as well as chronic diseases like diabetes and thyroid disease. Further studies with more participants are required, especially in summer, and it is important to conduct dry eye tests to better evaluate the prevalence of DES.
AUTHORS’ CONTRIBUTIONS
BHA: Supervision, Methodology, Software, Project administration. AAA 1: Literature review, Manuscript writing, Data collection, Reviewing, and Editing. AAA 2: Resources, Visualization. AAA 3: Investigation, Formal analysis. TWA: Literature review, Manuscript writing, Data collection, Reviewing, and Editing.
All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study design and protocol were approved by the local Institutional Review Board with the number: SUCOM/LIRB/2019-07.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All participants were given an explanation of the aims and objectives of the study through the questionnaire published on the website that contained informed consent.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were followed for this study.
AVAILABILITY OF DATA AND MATERIALS
The study data and materials are not publicly available due to the confidentiality and privacy of the participants.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors are thankful to Shaqra University, Ministry of Education, Kingdom of Saudi Arabia, for providing a platform to encourage research and development among the students, staff, and society.

