All published articles of this journal are available on ScienceDirect.

Toric Implantable Phakic Contact Lens in the Correction of Stable Keratoconus after Corneal Collagen Crosslinking
Abstract
Background:
The study aims to evaluate the safety profile and efficacy of toric Implantable Phakic Contact Lens (IPCL) in patients with stable keratoconus after corneal collagen crosslinking (CXL).
Methods:
A prospective interventional case series study involving 30 keratoconic eyes between 22 to 39 years of age implanted with toric IPCL 6 months after CXL. The refractive error, visual acuity, corneal endothelium, intraocular pressure (IOP), and adverse effects were observed for 12 months following the implantation.
Results:
The preoperative mean for the sphere was approximately -8.3±3.6, which improved postoperatively by -0.58±0.23 after 1 month, -0.48±0.19 after 3 months, -0.36±0.18 after 6 months, and -0.35±0.2 after 12 months respectively. About the cylinder, the preoperative mean for the cylinder was approximately -3.4±1.6, which improved postoperatively by -1.06±0.3 after 1 month, -0.76±0.19 after 3 months, -0.48±0.28 after 6 months and -0.53±0.12 after 12 months, respectively. The preoperative BCDVA was 0.34±0.13, which increased postoperatively to 0.18±0.11 after 12 months. The mean values for IOP were 14.5±1.5 mm Hg, 15.1±2.09 mm Hg, 13.8±2.2 mmHg, 13.3±1.7 mm Hg, 13.1±1.6 mm Hg at preoperative period, 1 month, 3 months, 6 months and 12 months postoperatively. The mean preoperative endothelial count was 2912.9±111.1 per square millimeter, 2854.7±113.2 cells per square millimeter after 6 months, and 2829.0±112.2 cells per square millimeter after 12 months.
Conclusions:
Toric IPCL is a safe approach for treating residual refractive errors, particularly astigmatism, after 6 months of CXL in patients with stable KCS.
1. INTRODUCTION
Keratoconus (KCS) is a chronic non-inflammatory corneal thinning condition resulting in myopia and irregular astigmatism leading to impairment of the visual acuity with a substantial negative impact on the quality of life due to the young age of most patients [1-3]. To stop the disease progression, corneal collagen cross-linking (CXL) may be used effectively, but visual acuity following CXL remains poor. Additional methods are needed to improve the vision in patients intolerant to rigid gas permeable contact lenses after CXL [1-2].
Intracorneal ring segment implantation (ICRS), phakic intraocular lenses (pIOL) and photorefractive keratectomy (PRK) are options for visual rehabilitation and can be all combined with CXL [4-6]. ICRS implantation is used in patients with poor best-corrected visual acuity [7-10]. The mild refractive error could be corrected by PRK [4, 5], while pIOL could be used to correct moderate to severe ametropia in a patient with good best-corrected visual acuity [6, 7].
The IPCL V2.0 TORIC (Caregroup, India) is a single piece posterior chamber phakic IOL, made from reinforced hybrid hydrophilic acrylic material to ensure long-term performance and can be inserted through a 2.8 mm corneal incision into the eye. The IPCL V2.0 TORIC can be used to correct myopia up to -30D with cylinders up to 10 D. The toric IPCL is customized according to the size and shape of each eye.
In our study, we present an interventional case series to determine the safety profile and efficacy of the new form of posterior chamber phakic IOLs for correction of myopia and/or astigmatism in patients of KCS who already underwent CXL.
2. MATERIALS AND METHODS
A prospective interventional case series study was performed from May 2020 to December 2021 in the Roaa Laser Vision Correction Center, International Eye Centre, and Minia University hospital. Toric IPCL was implanted in a total of 30 keratoconic eyes after 6 months of CXL. Written consent was obtained from all patients after receiving a detailed description of this modality of treatment. The study was accepted by the University of Minia's ethical committee.
The inclusion criteria were the age of more than 18 years and less than 40 years withthe absence of any history or physical signs of ocular disease other than KCS and myopia, significant improvement in best- corrected distance visual acuity (BCDVA) with their own refraction, stable refraction for at least 6 months after CXL (change in 2 subjective refractions within ±0.50 D of the spherical equivalent 3 months apart), K max ≤55, clear central cornea, internal anterior chamber depth (ACD) at least 3.00 mm, and normal intraocular pressure (IOP) by Tonopen (Reichert, Inc. USA). Endothelial cell count is related to age and the anterior chamber depth by specular microscopy (Tomey EM-3000, Tomey Co, and Japan). The Pentacam (Oculus Optikgeräte GmbH, Wetzlar, Germany) was used for diagnosis of KCS, measurement of keratmetric readings, internal ACD and pachymetry and all eyes had grade I or II KCS according to the Amsler-Krumeich classifification.
Exclusion criteria were the presentation of autoimmune disorders, Diabetes Mellitus, and other ophthalmic problems, except keratoconus, such as corneal opacification, uveitis, cataract, glaucoma, diabetic retinopathy, and the central endothelial cell count of less than 2000 cells/mm2 by specular microscopy, central corneal thickness of less than 450 µm, single eye patients and pregnant and lactating females.
Manifest and cycloplegic refraction, ACD, keratometric readings, and pachymetry measured by Pentacam and white-to-white (WTW) using a Castroviejo caliper (Ambler Surgical, Germany), were the data required for toric IPCL calculation. The software IPCL power choice of Care group Surgical was used for the calculation of the IPCL power.
The IPCL V 2.0 (Caregroup, India) is intended to be implanted behind the iris with the haptic zone resting on the ciliary sulcus. Its design has 6 haptics to increase stability, 2 holes in the peripheral portion from the upper zone and 4 holes outside the optical zone. This facilitates the cartridge loading and unfolding inside the eye. The IPCL has an additional central hole (380 micrometers), which reduces scattering and glare, allows easy alignment and aqueous humour circulation, and eliminates the need for the previous iridotomy. The diameter range of the optic is from 5.75 to 6.20 mm and 11.0 mm to 14.00 mm overall diameter (with 0.25 mm steps). Data is available from the Official lens Brochure, available from Care Group; (http://caregroupiol.com/products/phakic-lenses /ipcl/).
2.1. Surgical Procedure
All Toric IPCL implantation surgeries were performed under general anesthesia by the same surgeon (M.S) using V 2.0 IPCL design. Tropicamide 1% (Alcon Lab, Inc, Fort Worth, TX) was used for mydriasis every 10 minutes for at least 30 minutes. To avoid cyclotorsion, the zero horizontal axis was detected at the slit-lamp in the upright position. Loading of the IPCL was done before opening the eye. The cartridge was opened and filled with saline and hydroxypropyl methylcellulose (HPMC). Using McPherson forceps, the IPCL was gently held from the container near the haptic. After detection of its orientation, the IPCL was inserted in the cartridge and the cartridge was put in the injector. A 2.8 mm clear temporal corneal incision was performed and the anterior chamber was partially filled with HPMC. The IPCL was slowly injected into the AC for detection of the orientation. The four footplates were placed under the iris plane by gentle pressure on them. Detection of the exact orientation of the toric IPCL in the horizontal axis using the landmarks on the surface of the IPCL. Miosis was done by Miochol-E (acetylcholine chloride intraocular solution) 1:100 with Electrolyte Diluent (Novartis, Switzerland). Irrigation aspiration of the viscoelastic was performed and wound hydration was performed.
Postoperatively, a topical antibiotic as moxifloxacin HCL 0.5% was used for 2 weeks, a topical steroid as prednisolone acetate ophthalmic suspension 0.5% was used and tapered over 1 month, and sterile ophthalmic ointment containing tobramycin 0.3% and dexamethasone 0.1% was used at night.
The patients were evaluated for 12 months for the uncorrected distant visual acuity (UDVA), corrected distant visual acuity (CDVA), slit-lamp examination, manifest and cycloplegic refraction, the central endothelium count, IOP, and any complications.
2.2. Statistical Analysis
Data was revised for its completeness and consistency. The statistical package version 20 of IBM SPSS (Chicago, USA) was used for data entry. The time course of changes was analyzed by one-way variance analysis (ANOVA), with the Dunnett test for multiple comparisons. To compare the pre- and post-surgical data, the Wilcoxon signed-rank test was used for statistical analysis. Unless otherwise indicated, the results are expressed as mean±SD, and a value of p<0.05 was considered statistically significant.
3. RESULTS
3.1. Demographic Data
30 eyes (14 females and 16 males) of keratoconic patients were included in the study; the mean age was 27.8±6.09 years (range: 22 to 39 years). All cases had a unilateral intervention (Table 1).
Table 1.
| Age in years: mean ±SD (range) | 27.8±6.09 (22-39) |
| Sex: n (%) | |
| Males | 16 (53.3%) |
| Females | 14 (46.7%) |
3.2. Refractive Outcome
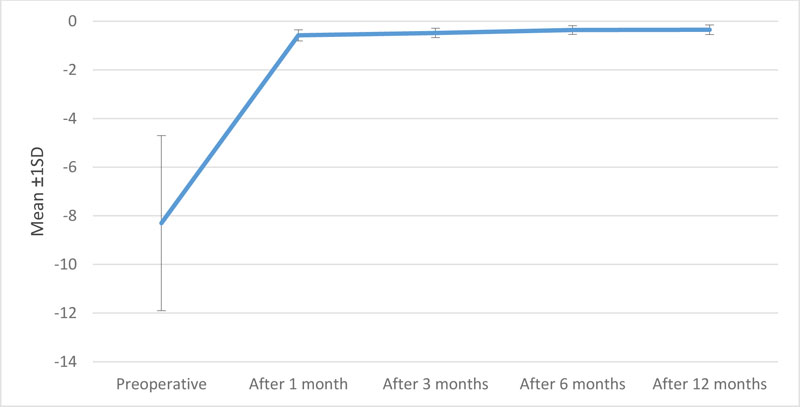
About the sphere, the preoperative mean was about -8.3±3.6, which improved postoperatively-0.58±0.23 after 1 month, -0.48±0.19 after 3 months,-0.36±0.18 after 6 months and -0.35±0.2 after 12 months (Table 2 and Fig. 1).
| Preoperative | After 1 month | After 3 months | After 6 months | After 12 months | |
|---|---|---|---|---|---|
| Mean ±SD | -8.3±3.6 | -0.58±0.23 | -0.48±0.19 | -0.36±0.18 | -0.35±0.20 |
| p-value | |||||
| Preoperative | <0.001 | <0.001 | <0.001 | <0.001 | |
| After 1 month | <0.001 | <0.001 | <0.001 | ||
| After 3 months | <0.001 | <0.001 | |||
| After 6 months | 0.161 | ||||
| After 12 months |
About the cylinder, the preoperative mean was about -3.4±1.6, which improved postoperatively -1.06±0.3 after 1 month, -0.76±0.19 after 3 months,-0.48±0.28 after 6 months and -0.53±0.12 after 12 months (Table 3 and Fig. 2).
| Preoperative | After 1 month | After 3 months | After 6 months | After 12 months | |
|---|---|---|---|---|---|
| Mean ±SD | -3.4±1.6 | -1.06±0.30 | -0.76±0.19 | -0.48±0.28 | -0.53±0.12 |
| p-value | |||||
| Preoperative | <0.001 | <0.001 | <0.001 | <0.001 | |
| After 1 month | <0.001 | <0.001 | <0.001 | ||
| After 3 months | <0.001 | <0.001 | |||
| After 6 months | 0.312 | ||||
| After 12 months |

3.3. Visual Scuity
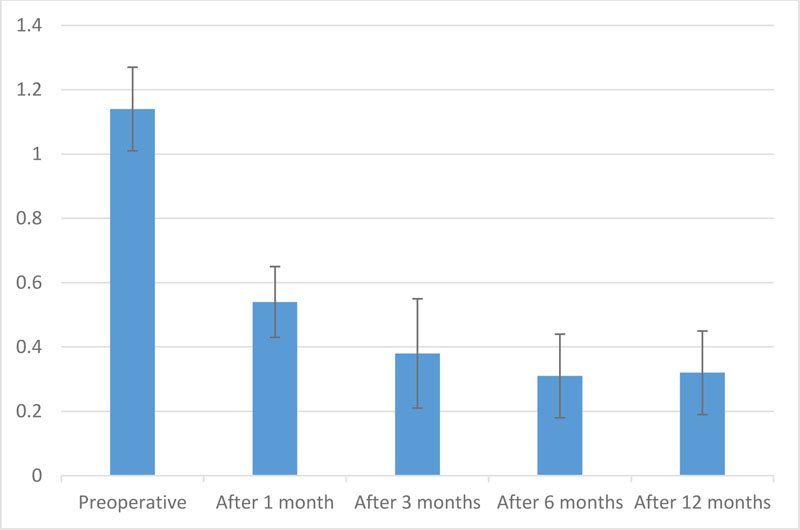
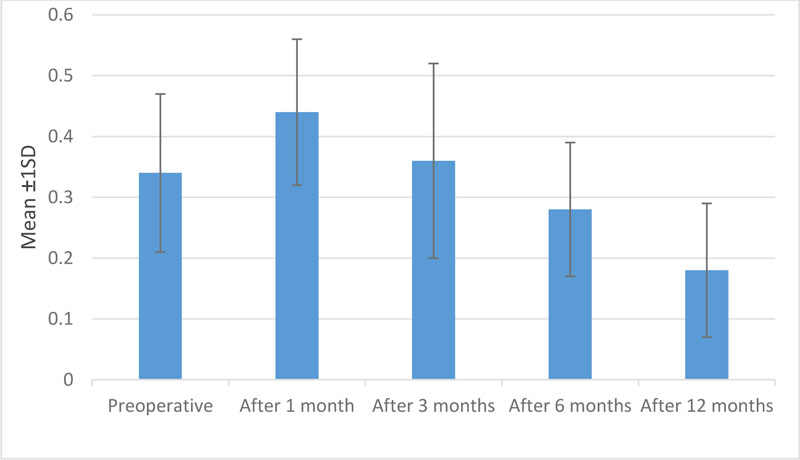
The preoperative UCDVA was 1.14±0.13, which improved postoperatively to 0.32±0.13 after 12 months. The changes were illustrated in the Table 4 and Fig. (3). The preoperative BCDVA was 0.34±0.13, which improved postoperatively to 0.18±0.11after 12 months. The changes are illustrated in Table 5 and Fig. (4).
| Preoperative | After 1month | After 3 months | After 6 months | After 12 months | |
|---|---|---|---|---|---|
| Mean ±SD | 1.14±0.13 | 0.54±0.11 | 0.38±0.17 | 0.31±0.13 | 0.32±0.13 |
| p-value | |||||
| Preoperative | <0.001 | <0.001 | <0.001 | <0.001 | |
| After 1 month | <0.001 | <0.001 | <0.001 | ||
| After 3 months | <0.001 | 0.001 | |||
| After 6 months | 0.161 | ||||
| After 12 months |
| Preoperative | After 1 month | After 3 months | After 6 months | After 12 months | |
|---|---|---|---|---|---|
| Mean ±SD | 0.34±0.13 | 0.44±0.12 | 0.36±0.16 | 0.28±0.11 | 0.18±0.11 |
| p-value | |||||
| Preoperative | <0.001 | 0.161 | <0.001 | <0.001 | |
| After 1 month | <0.001 | <0.001 | <0.001 | ||
| After 3 months | <0.001 | <0.001 | |||
| After 6 months | 0.161 | ||||
| After 12 months |
3.4. IOP
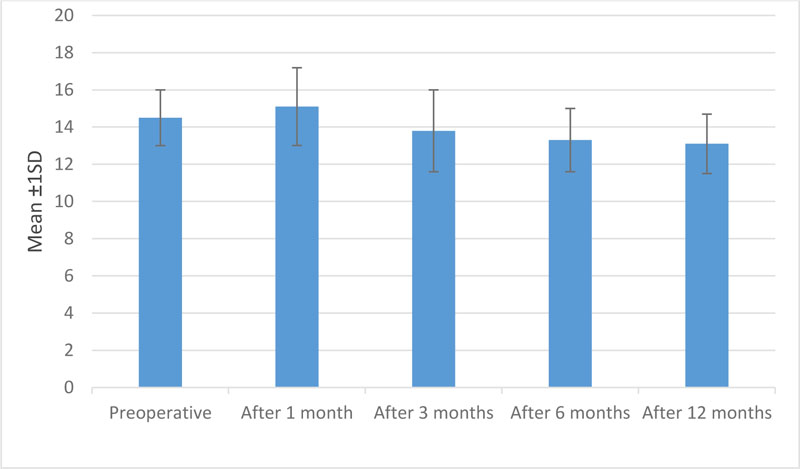
The mean values were 14.5±1.5 mm Hg, 15.1±2.09 mm Hg, 13.8±2.2 mmHg, 13.3±1.7 mm Hg,13.1±1.6 mm Hg in the preoperative period, after 1 month, after 3 months, after 6 months and after 12 months postoperatively. The changes are illustrated in Table 6 and Fig. (5).
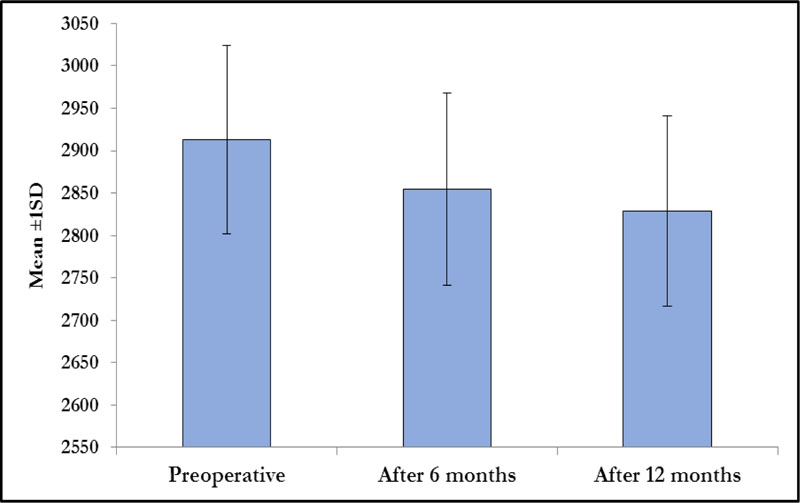
3.5. Endothelial Cell Count
The mean endothelial preoperative count was 2912.9±111.1 per square millimeter, 2854.7±113.2 cells per square millimeter after 6 months and 2829.0±112.2 cells per square millimeter after 12 months. The changes are illustrated in Table 7 and Fig. (6).
Table 6.
| Preoperative | After 1 month | After 3 months | After 6 months | After 12 months | |
|---|---|---|---|---|---|
| Mean ±SD | 14.5±1.5 | 15.1±2.09 | 13.8±2.2 | 13.3±1.7 | 13.1±1.6 |
| p-value | |||||
| Preoperative | 0.177 | 0.060 | 0.005 | 0.004 | |
| After 1 month | 0.011 | <0.001 | <0.001 | ||
| After 3 months | 0.307 | 0.206 | |||
| After 6 months | 0.645 | ||||
| After 12 months |
| Preoperative | After 6 months | After 12 months | |
|---|---|---|---|
| Mean ±SD | 2912.9±111.1 | 2854.7±113.2 | 2829.0±112.2 |
| p-value | |||
| Preoperative | <0.001 | <0.001 | |
| After 6 months | <0.001 | <0.001 | |
| After 12 months | <0.001 | <0.001 |
4. DISCUSSION
This study was done in Roaa Laser Vision Correction Center, International Eye Centre, and Minia University hospital in 30 keratoconic eyes; the toric IPCL was implanted 6 months after CXL, which was done first to stabilize the progression of the disease. For the diagnosis of KCS, Computed slit-scanning videokeratography of the anterior and posterior corneal surfaces, keratometric readings and pachymetry were used. Being a refractive surgery, the inclusion criteria are patients over 18 years of age with stable refraction, no cataract, no glaucoma, clear cornea and no retinal pathology. Patients with cataracts, glaucoma, corneal opacity, uveitis and abnormal retinal pathology were excluded.
All patients in our study had grade I or II KCS according to the Amsler-Krumeich classification and we excluded patients with progressive KCS who will get no benefit from IPCL surgery and are unfit for CXL.
CXL increases the corneal stiffness by inducing more corneal collagen crosslinks of the cornea, and the remaining refractive errors are still the remaining issue [11]. There is a big research gap regarding the residual refractive error correction either by spectacles, hard contact lenses or phakic IOLs.
When reviewing the previous literature, we found that CXL was done and waited at least 6 months for phakic IOLs implantation after CXL because of the significant effect of CXL in keratometric values from 0.92 to 2.10 D and decrease of mean spherical equivalent refraction from 0.93 to 1.42 D. So before implanting toric IPCL, we wait 6 months after CXL to consider for corneal stabilization and for accurate measurement of the toric IPCL power calculation. This comes in agreement with previous studies which implanted other toric phakic IOLs as toric implantable collamer lenses (TICL) as Fadlallah et al., 2013 [9] and Antonios et al., 2015 [12] disagree with Shafik et al., 2014 [10], who implanted TICL after 12 months of CXL.
The toric IPCL power calculation parameters were the refraction, K readings, ACD, pachymetry and WTW measurement. All refractions were based on refined refraction using trial lenses, and the axis of astigmatism was chosen according to the best visual acuity obtained while rotating the astigmatism trial axis as the findings of the autorefractometer regarding the manifest refraction and axis of astigmatism were not always accurate in patients of KCS. The target was emmetropia in all cases. The lens size was based on horizontal WTW and ACD. WTW was measured manually by caliper (Castroviejo caliper, Ambler Surgical, Germany) by a single surgeon (M.S) at least three times (three values) to avoid visually significant complications post-surgery. ACD was measured by Pentacam and the internal ACD was measured from the corneal endothelium to the anterior lens capsule.
In our study, 30 eyes were implanted with the IPCL V2.0 TORIC design, which has a central hole in the optic of about 380 microns for proper aqueous flow without prior iridotomy. This hole is designed to minimize the scattering of light and glare and does not induce significant visual disturbances. The old design, V1.0, has the same design as V2.0 but without a central hole, so PI was necessary with this design. This design is not available nowadays.
In the early postoperative period, the IOP was increased in some cases, mostly due to some retained viscoelastic.
Our results agreed with a study done by Doroodgar F et al., 2019 [13], who implanted toric IPCL in 28 keratoconic eyes after 6 months of CXL and followed up to 6 months after IPCL implantation.
In our study, during the follow up period, there were no cases of chronic increased postoperative IOP or anterior subcapsular cataract.
With regard to the refractive outcome, all eyes were within 0.5 D of the intended spherical equivalent and we obtained satisfactory results. Also, the values of astigmatism decreased significantly to nearly clinically values of no importance.
Other studies who studied toric ICL (STAAR surgical inc., Switzerland) implantation after CXL in keratoconus are Fadlallah et al.,2013 [9], who studied 16 eyes of 10 patients with keratoconus with CXL at first, then toric ICL implantation after 6 months, Shafik et al., 2014 [10] who studied keratoconic 16 eyes with CXL at first then toric ICL implantation after 12 months and Antonios et al., 2015 [11] who implanted Visian toric ICL after 6 months of CXL in 30 eyes of 19 patients with progressive keratoconus.
There were other studies about posterior chamber phakic IOls in keratoconus but without CXL, as Alfonso et al.,2010 [14], who implanted TICL in 30 keratoconic eyes of 21 patients in early stage keratoconus without CXL, Kamiya et al.,2011 [15] implanted TICL in 27 keratoconic eyes of 14 patients in mild keratoconus without CXL, Hashemian et al.,2012 [16] implanted TICL in 22 keratoconic eyes of 14 patients without CXL, and Kamiya et al.,2015 [17] implanted TICL in 21 keratoconic eyes of 11 patients with early keratoconus without CXL.
Regarding other phakic IOLs, Budo et al., 2005 [18] implanted iris-fixated toric phakic IOL with a higher reduction in the spherical error (87.4%) than the astigmatic error (64.5%), suggesting that spherical errors are highly predictable but astigmatic errors were less predictable. Angle-supported phakic IOLs were implanted by Leccisotti and Fields 2003 [19], but a 5.5-mm sclerocorneal incision did not improve astigmatism. Iris-supported phakic IOL was implanted by Kato et al., 2011 [20], who reported that about 86% of patients said they were ‘satisfied’ or ‘very satisfied’1 year postoperatively. Guell et al., 2012 [21] implanted toric Artiflex/ Artisan after CXL with no risk of IOL rotation after surgery due to the elevation system on the iris, which was an advantage over toric posterior chamber phakic IOLs. Alió et al., 2014 [22] found no statistical variation in the safety and stability results between the iris-supported and posterior chamber phakic IOLs.
Other choices for keratoconus therapy are the use of ICRS and CXL, but with less reduction in myopia and astigmatism than with toric phakic IOLs. Phakic IOL could be implanted after ICRS by Jarade et al., 2013 in a two-step procedure for treating progressive keratoconus [23].
Refractive lens exchange (RLE) was done by Leccisotte 2006 [24] in keratoconus with low corneal astigmatism, but the results were unsatisfactory as 32% of patients needed IOL exchange due to IOL miscalculation in addition to the loss of accommodation.
CONCLUSION
Toric IPCL is a safe approach for treating residual refractive errors in patients with stable keratoconus, particularly, astigmatism, after 6 months of CXL. Toric IPCL is a good alternative to toric ICL (which is more expensive than toric IPCL), especially in our country.
LIMITATIONS
Our study had some limitations as the small sample of patients with a short duration of follow-up. Also, the lack of comparison with toric ICL.
LIST OF ABBREVIATIONS
| IPCL | = Implantable Phakic Contact Lens |
| CXL | = Collagen Crosslinking |
| KCS | = Keratoconus |
| ACD | = Anterior Chamber Depth |
| IOP | = Intraocular Pressure |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Institutional Review Board and Research Ethics Committee of Minia University, Egypt, under approval no. (628-6/2020).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written consent was obtained from all patients after receiving a detailed description of the nature of this modality of treatment.
AVAILABILITY OF DATA AND MATERIALS
The data in the present study are available from the corresponding authors [M.M] upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

