All published articles of this journal are available on ScienceDirect.

Five Consecutive Cases of Liquefied Aftercataract: Impact of Nd:YAG Laser Capsulotomy on Refraction and High-Order Aberrations
Abstract
For five consecutive eyes from five patients with liquefied aftercataract, Nd:YAG laser treatment significantly reduced high-order aberrations. Two eyes showing a reduction in positive spherical-like aberrations after treatment showed a postoperative myopic shift, while three eyes showing no change in spherical-like aberrations demonstrated hyperopic or only a slight myopic shift.
TO THE EDITOR
Liquefied aftercataract (LAC) is a rare condition characterized by a liquefied, milky white substance accumulating between the optic of the intraocular lens (IOL) and the posterior lens capsule [1]. LAC can occur when the anterior capsular opening made by continuous curvilinear capsulorhexis—an important technique of modern cataract surgery—is occluded with the IOL optic. Although LAC can result in decreased vision [1], knowledge of high-order aberrations generated by LAC is scarce. We measured refraction and high-order aberrations altered by Nd:YAG laser posterior capsulotomy for LAC, surmising the influence of LAC on refraction of the eye.
Informed consent was obtained from all subjects prior to participation, and the study adhered to the tenets of the Declaration of Helsinki. No institutional review board approval was required for this study because cataract surgeries and Nd:YAG laser posterior capsulotomy have been widely performed.
Five consecutive eyes from five patients who underwent phacoemulsification and IOL insertion at Nikko Memorial Hospital were examined. All developed LAC with subjective visual symptoms after surgery and subsequently underwent Nd:YAG laser posterior capsulotomy between June and September 2010. LAC was defined as a distended posterior capsule and accumulation of a liquefied substance between the IOL and posterior capsule observed during slit-lamp examination. The clinical data of the patients are shown in Table 1. All IOL were biconvex-shaped and spheric. In each case, Healon® (Abbott Laboratories, Abbott Park, Ill, USA) was used as the ophthalmic viscosurgical device. Before each Nd:YAG laser treatment, we confirmed the absence of obvious anterior displacement and decentration or tilt of the IOL with the slit-lamp, and established that intraocular pressure was within the normal range.
Clinical Data From 5 Patients (5 Eyes) with Liquefied Aftercataract
| Patient No., Age (Yrs), Sex | Complications/Remarks | Preoperative AL1 (mm) | Intraocular lens | Time to capsu lotomy (yrs) | BCVA2 (LogMAR) (Pre-/Postcapsulotomy) | SERE3 (D) (Pre-/Postcapsulotomy) | SLA4 (µm) (Pre-/Postcapsulotomy) | CLA5 (µm) (Pre-/Postcapsulotomy) | Map Pattern of SLA4 |
|---|---|---|---|---|---|---|---|---|---|
| 1, 84, F | PDR6 | 22.88 | VA-60BB, HOYA | 5.1 | +0.4/+ 0.4 | -0.125/-0.25 | 0.141/0.126 | 0.572/0.482 | NCE† |
| 2, 73, F | Combined cataract surgery and PPV7 for BRVO8 | 23.70 | AR40e, AMO9 | 5.2 | +0.2/+0.2 | -1.125/-0.625 | 0.083/0.043 | 0.160/0.153 | NCE† |
| 3, 75, F | DM10 | 22.76 | MA60BM, Alcon | 8.2 | +0.1/0 | -0.675/-0.125 | 0.144/0.091 | 0.478/0.320 | NCE† |
| 4, 63, F | None | 25.25 | VA-60BB, HOYA | 4.3 | +0.2/+0.1 | -0.75/-1.375 | 0.211/0.121 | 0.372/0.327 | PAD‡ |
| 5, 62, F | PDR6 | 21.64 | YA-60BB, HOYA | 4.6 | +0.2/0 | -0.625/-0.875 | 0.165/0.109 | 0.318/0.257 | PAD‡ |
Map patterns of spherical-like aberrations were categorized into the
† NCE group (those showing no capsulotomy effect)
‡ PAD group (those showing a positive spherical aberration depressed by capsulotomy)
1 AL= axial length, measured using A-scan ultrasound
2 BVCA= best-corrected visual acuity
3 SERE= spherical equivalent refractive error
4 SLA= spherical-like aberration (4-mm diameter)
5 CLA= coma-like aberration (4-mm diameter)
6 PDR= proliferative diabetic retinopathy
7 PPV= pars plana vitrectomy
8 BRVO= branch retinal vain occlusion
9 AMO=Abbott Medical Optics
10 DM= diabetes mellitus.
Using OPD-Scan II version 2.10c (Nidek, Gamagori, Japan), corneal topography, autorefraction and high-order aberrations, as well as visual acuity, were measured immediately before and 1 month after capsulotomy. Examinations for refraction and aberrations were performed 30 minutes after instillation of 0.5% tropicamide and 0.5% phenylephrine. The maximum diameter for analysis of the aberrations was set at 4 mm, thus preventing disturbance by the iris.
Corneal topography analysis showed no asymmetrical or irregular astigmatism in any of the eyes. As shown in Fig. (1), based on map patterns of the spherical-like aberrations, patients were categorized as one of two types: those showing no obvious changes in aberrations (no capsulotomy effect group; NCE group), and those demonstrating an advanced wavefront component in the center, depressed as a result of capsulotomy (positive aberration depressed group; PAD group).
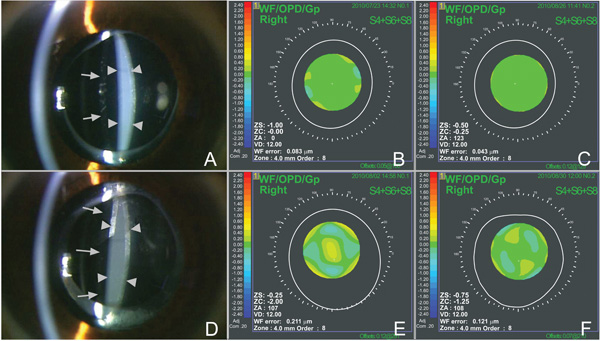
Case 2: Slit-lamp photograph taken before Nd:YAG capsulotomy (A), and map patterns of the spherical-like aberrations. No remarkable change was observed before (B) and after (C) treatment. Case 4: Slit-lamp photograph before treatment (D), and map patterns of the spherical-like aberrations before (E) and after (F) treatment. Preoperative positive aberrations decreased after treatment. Photographs show liquified aftercataracts (arrowheads) and anterior surfaces of the intraocular lenses (arrows).
Measured values for each of the 2 groups are shown in Table 1. After capsulotomy, best-corrected visual acuity (BCVA) was improved (logMAR change >0.1) in only one eye in the PAD group, and no eye showed a decrease in BCVA (logMAR change >0.1). The spherical equivalent refractive error was negatively altered by ≥0.25 D in the PAD group, while a positive or negative change <0.25D was observed in the NEC group. In all eyes, both spherical-like and coma-like aberrations significantly decreased (P=0.015 and 0.047, respectively; paired 2-tailed t test).
The OPD-Scan II employed in this study was based on the retinoscope principle for measuring aberrations [2]. The aberration values obtained by the OPD-Scan II were similar to those of the currently popular Hartmann-Shack wavefront sensor [2]. LAC was defined according to Miyake et al. [1] who classified LAC as late-onset postoperative capsular block syndrome (CBS), usually without high intraocular pressure or a shallow anterior chamber [3]. LAC development is thought to occur as a result of accumulation of proliferated residual lens cortex in the closed chamber behind the IOL optic, resulting in an osmotic gap that draws the aqueous humor into the chamber [1]. The incidence of LAC is reportedly 0.27% (3/1100) as late-onset CBS [4]. Because most of our patients finished follow-up by 3 months after cataract surgery, except in the case of particular complications, we were not able to estimate the incidence in the present study.
Although Nd:YAG laser posterior capsulotomy for postoperative posterior capsule opacity is known to reduce high-order aberrations [5], no report has yet to determine the aberrations derived from LAC. Here, Nd:YAG laser posterior capsulotomy for LAC significantly decreased both spherical-like and coma-like aberrations, suggesting that LAC increases high-order aberrations. Although Nd:YAG laser treatment does not always improve visual acuity, it does seem to improve visual quality when assessed in terms of high-order aberrations.
The PAD group, which showed a decrease in positive spherical-like aberrations after capsulotomy, became myopic after treatment, suggesting that LAC had a hyperopic effect in this group. Accumulation of a high concentration of materials in the closed space between the IOL and posterior capsule may give the cavity a concave-lens effect as reported by Shah et al. [6] as well as positive spherical-like aberrations. In contrast, the NCE group, which showed no alterations in positive map patterns for spherical-like aberrations after capsulotomy, showed no obvious refractive change or became only slightly hyperopic after treatment. In this group, we surmised that the lower concentration did not result in a lens-like effect, resulting in myopic change due to anterior shift of the IOL, the mechanism of early-onset CBS [3].
Although we demonstrated that the refractive characters of LAC vary, the PAD group seemed to become more myopic than the NCE group. The direction of refractive change after capsulotomy may therefore be predicted by examining preoperative map patterns for spherical-like aberrations.
Our study had certain limitations. The number of patients was limited; a larger study group might reveal a significant relationship between map-patterns for spherical-like aberrations and refractive change resulting from capsulotomy. In addition, quantitative analysis of turbidity of the LAC and measurement of anterior-chamber depth might help clarify the mechanism proposed here.
In summary, Nd:YAG laser posterior capsulotomy for LAC in five eyes significantly reduced high-order aberrations although it did not always improve visual acuity. Two eyes with a reduction in positive spherical-like aberrations after capsulotomy showed a postoperative myopic shift, whereas three eyes with no change in spherical-like aberrations demonstrated a hyperopic or only slight myopic shift. These findings suggest that LAC can simultaneously cause a hyperopic shift and positive spherical-like aberrations.
ACKNOWLEDGEMENT
Declared none.
CONFLICTS OF INTEREST
Declared none.

