All published articles of this journal are available on ScienceDirect.

Incidence of Retinal Pigment Epithelial Tears and Associated Risk Factors After Treatment of Age-Related Macular Degeneration with Intravitreal Anti-VEGF Injections§
Authors Info & Affiliations
Abstract
Purpose :
To study the incidence and risk factors for retinal pigment epithelium tears following intravitreal anti-vascular endothelial growth factor (VEGF) injections.
Methods :
Retrospective longitudinal study. 4027 intravitreal anti-VEGF injections in 628 patients (676 eyes) for choroidal neovascularisation associated with age related macular degeneration in a period of 18 months were studied.
Results :
Seventeen patients (mean age 83.95±5.84) developed retinal pigment epithelium tears. The incidence rate was 0.4%. Fibrovascular pigment epithelium detachment (PED) was previously observed in all cases. In 88 % (15/17) of AMD patients that had a RPE tear, PED height was found to be less than 400 microns at presentation. In 5 of 7 patients with RPE tear grade <4, continuing of anti-VEGF treatment resulted to improvement of visual acuity.
Conclusion :
Critical risk factors for RPE tears are presence of PED as well as advanced age. Visual improvement appears to depend more on the extent and location of the RPE tear and less on the PED height.
INTRODUCTION
Retinal pigment epithelium (RPE) tears are defined as well-demarcated areas of bare choroid, visible immediately adjacent to a hyper pigmented area which represents the redundant and retracted RPE. (Fig. 1A) In optical coherence tomography (OCT), RPE tears are defined as an interruption of the hyper reflective RPE layer with elevation of the torn RPE flap and increased choroidal depth signals posterior to the RPE tear (Fig. 1B).
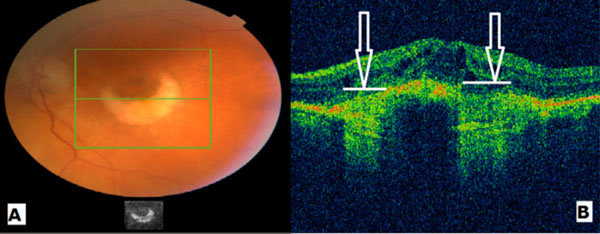
A: Color fundus photograph showing an RPE tear. B: OCT of the same patient illustrating clearly the increase of the choroidal depth signal in areas of RPE absence (white arrows).
Since they were first described by Hoskin et al. [1], tears of the RPE have been recognized increasingly as a cause of severe central visual loss in age related macular degeneration (AMD). As a general rule, RPE tears are part of the natural history of a pigment epithelial detachment (PED) that has developed as a result of occult choroidal neovascularization, retinal angiomatous proliferation, or polypoidal choroidal vasculopathy [2, 3]. In addition, tears may occur spontan-eously, following photodynamic laser treatment, laser photocoagulation, and YAG laser posterior capsulotomy [4-6]. RPE tears are classified according to the criteria of Sarraf et al. grade 1 (diameter smaller than 200 μm), grade 2 (diameterbetween 200 μm and 1 disc diameter), grade 3 (diameter > 1 disc diameter) and grade 4 (Grade 3 tears that involve the foveal centre) [7]. RPE tears have also been described in eyes with PED after anti-vascular endothelial growth factor (VEGF) treatment [8-10]. Reported incidence of RPE tears in the literature ranges from 1.8% to 27%, in both natural history and interventional series [11]. The overall incidence of RPE tears was even lower (0.7-5.1%) in the phase III randomised multicenter clinical trials of ranibizumab for the treatment of neovascular AMD (MARINA, ANCHOR and PIER trials) [12]. Several studies have also shown risk factors associated with RPE tears such as height of PED on OCT and size of the baseline PED lesions [13]. Recent attention has been paid to the suspicion that RPE tears occur more commonly after anti-VEGF therapy, but this relationship has not been clearly established. Patients with pre-existing subfoveal tears of the RPE have been excluded from prospective trials of anti-VEGF therapy and hence their response to subsequent anti-VEGF therapy is not well-understood.
In the present study we describe the incidence rate and risk factors for RPE tears following intravitreal anti-VEGF treatment in a single institution. In addition we investigate the effect of continuing anti-VEGF treatment after RPE tear development.
METHODS
A longitudinal, retrospective study was undertaken of the medical records of patients who attended the retina service at the Leicester Royal Infirmary between May 2010 and December 2011. Eligibility criteria for the study included: identification of occult subretinal CNV on indocyanine green angiography (ICGA), treatment with intravitreal injections of ranibizumab (Lucentis; Genentech, Inc, South San Francisco, CA) or bevacizumab (Avastin; Genentech) and follow up of at least 12 months. Exclusion criteria were: other previous treatment (laser, photodynamic therapy), ocular abnormalities other than AMD affecting visual function or treatment outcome. The treatment plan included a 3-monthly loading phase of intravitreal injections. Further injections provided depending on the OCT detection of subretinal fluid (SRF), intraretinal fluid (IRF), and persistence or recurrence of PED. Patients were evaluated on a regular basis (maximum intervals of 3 months) for at least 12 months.
RPE tears were diagnosed based on fundus examination, Spectral Domain optical coherence tomography (OCT) (3D OCT-1000, Topcon Corporation, Tokyo, Japan), and fundus fluorescein angiography (FFA). RPE tears were then classified according to the criteria of Sarraf. In our service, intravitreal anti-VEGF injections were continued even after a RPE tear development, except from grade 4 tears.
Data were collected retrospectively, and the completed data forms were analyzed with Microsoft Excel 2010 for Windows (Microsoft Corporation, Redmond, WA, USA).
RESULTS
A total of 628 patients (mean age 80.9±7.3 years), 676 eyes and 4027 injections were analysed. RPE tears developed in 17 cases (0.4%) (12 women). Mean age of this group of patients was 83.94±5.84 years. 14/17 of the patients that developed RPE tear were over 80 years old.
15/17 patients had a PED height of less than 400 microns at presentation and developed RPE tears within 6 months after the intravitreal anti-VEGF treatment initiation. 14 patients developed RPE tear earlier than the sixth intravitreal injection.
The visual outcome was poor in 10 patients, as they had Grade 4 RPE tears. The remaining 7 patients had Grade 1-3 RPE tears and visual acuity slightly improved in 5 of them with the continuation of their anti-VEGF treatment (Table 1).
Visual acuity (LogMAR) of patients that developed RPE tear and continued anti-VEGF treatment.
| Patient | VA (at RPE Tear) | VA (After 12 Months) | Outcome |
|---|---|---|---|
| 1 | 0.6 | 0.6 | Stable |
| 2 | 1.0 | 0.84 | Improved |
| 3 | CF | 0.82 | Improved |
| 4 | 0.6 | 1.0 | Worsened |
| 5 | 1.12 | 0.96 | Improved |
| 6 | 1.2 | 0.92 | Improved |
| 7 | 0.8 | 0.64 | Improved |
DISCUSSION
In terms of visual prognosis in RPE tears, even if the short-term visual prognosis is relatively unchanged by RPE tears, they are associated with a slow decrease in vision in the long term, often resulting in a severe visual disability. RPE tears are associated with subretinal bleeding and development of disciform scars that lead to this poor visual prognosis. However, few reports have described that anti-VEGF can improve the outcome of this condition [14-17]. Repopulation of the RPE after pigment epithelium tear has been described as one potential avenue for post-tear visual gains by Peiretti et al. [18], in a patient with RPE tear and polypoidal choroidal neovascularisation. There are suggestions that persistent anti-VEGF therapy is important to continue to suppress the neovascular activity in cases of RPE tears grade 3 or lower [19-21]. Therefore, in these cases the possible clinical benefits tend to appear at 3 months’ time. For grade 4 RPE tears, macular surgery with macular translocation or an RPE graft could be an option [22, 23]. It is debatable if a more aggressive or alternatively a more reserved treatment regime would result in better visual results.
The overall incidence rate reported in our study (0.4%) was comparable to the reported literature. Presence of fibrovascular PED appears to be a significant risk factor for the development of RPE tears in AMD. Large PED diameter and vertical height on OCT (>400 μm) have been shown to increase the risk of RPE tear. However, our study shows that 88% (15/17) of the RPE tears developed from PEDs with height less than 400 μm. This finding is very interesting and implies that PED height may not be such a decisive risk factor for RPE tears development. Since the mean age of our cases was over 80 years, one can hypothesize that the integrity of the RPE is an additional factor leading to tearing of older people compromised retinal pigment epithelium. Saraff’s RPE tear classification system comprises a solid base for the study of the entity and in our opinion additional parameters as age and RPE thickness could attribute to an even more complete explanation and prognosis of this devastating condition.
It has also been shown that RPE tears always developed relatively close to the initiation of the anti-VEGF treatment (1-3 months). The mean number of injections before the diagnosis of a new RPE tear in our study was 7.2. RPE tears might be initiated during anti-VEGF therapy, as a result of tractional forces at the level of RPE [24]. The time association between the development of RPE tears and the initiation of anti-VEGF treatment cannot prove a causative relation, but it should be taken into consideration as a complication of the treatment.
Further studies are needed to address when patients with RPE tears should receive treatment. Retreatment decisions are complex, given that fluid leakage may occur not only due to choroidal neovascular activity, but also secondary to the absence of RPE, which functions to pump out fluid from the subretinal space.
A workable limitation of the current study is its retrospective nature. Nevertheless, the study was conducted in a large referral center where the accuracy of data is assured. Another limiting factor could be considered the inclusion of two eyes for some patients. However, all of our cases were unilateral so no further analysis was needed.
In conclusion, this study demonstrates that a considerable risk factor for RPE tears development is a previously diagnosed PED. In the majority of our cases, PED height was not as critical factor as the patient’s age, showing a possible age dependent resistance of the RPE to stretching caused by the PED.
Large randomised controlled clinical studies may be necessary to establish the burden of possible risk factors as well as to define the optimum management after a retinal pigment epithelium tear in patients with age related macular degeneration.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

