All published articles of this journal are available on ScienceDirect.

Comparison of Standard and Total Keratometry Astigmatism Measured with three Different Technologies
Abstract
Purpose:
To compare the keratometric and total corneal astigmatism measures provided by three different technologies as well as to assess the level of interchangeability among them.
Methods:
A Prospective, comparative study enrolling 94 eyes from 53 patients (age, 29-77 years) was carried out. All participants were patients with the diagnosis of cataract or patients with a transparent crystalline lens but seeking surgical presbyopia correction. A complete eye examination was performed in all eyes, including corneal analysis with three different devices: IOL-Master 700 (Carl Zeiss Meditec), Cassini (i-Optics), and Pentacam (Oculus Optikgeräte GmbH). Interchangeability of standard and total keratometric readings (equivalent keratometric readings for Pentacam) and astigmatism measures with these three systems were evaluated with the Bland-Altman analysis.
Results:
Significantly higher standard and total keratometric readings were obtained with the IOL-Master compared to the other two systems (p<0.001). Likewise, a significantly higher magnitude of standard and total keratometric astigmatism was obtained with the Cassini system (p<0.001). Ranges of the agreement for corneal power measurements between devices varied from 0.58 D to 1.53 D, whereas they ranged from 0.46 D to 1.37 D for standard and total astigmatism measurements.
Conclusion:
Corneal power and astigmatism measures obtained with IOL-Master 700, Cassini, and Pentacam systems cannot be used interchangeably. The impact of these differences on the refractive predictability achieved with different types of intraocular lenses (IOL) should be evaluated in the future in order to define which is the best corneal evaluation approach for optimizing the IOL power calculations.
1. INTRODUCTION
Cataract surgery with toric intraocular lens (IOL) implantation is an effective option for visual rehabilitation in presbyopic or cataract eyes with pre-existing corneal astigmatism [1]. A critical issue for an optimized outcome with this type of implants is an adequate calculation of the astigmatic power required for the IOL that is going to be implanted [2]. This calculation is based on the magnitude and axis of corneal astigmatism considered, which can be measured and calculated using different devices and mathematical approaches [3]. The classical keratometric approach estimates the corneal astigmatism considering the cornea as a single dioptric surface separating two media, air and one fictitious medium represented by the keratometric refractive index [4]. Therefore, the contribution of the posterior corneal astigmatism to total corneal astigmatism is assumed to be negligible [4], but this has been demonstrated to contribute to clinically relevant errors [5, 6]. Specifically, the magnitude of posterior corneal astigmatism (PCA) has been demonstrated to be correlated with anterior corneal astigmatism (ACA) for patients with with-the-rule (WTR) astigmatism, but there was a weak and no correlation for oblique and against-the-rule (ATR) eyes, respectively [6]. Likewise, the magnitude and axis of PCA have been shown to vary significantly in the healthy cornea, especially when ATR ACA is present [7].
Different algorithms of correction of keratometric estimations of total corneal astigmatism have been developed to consider the potential contribution of PCA to the calculations of the power of toric IOLs, as well as the contribution of incision-induced posterior corneal astigmatism and effective lens position [3, 8-12]. For example, the Abulafia-Koch regression formula was developed to estimate the total corneal astigmatism according to some adjustments based on standard keratometry measurements [13]. Manufacturers of new topographic and tomographic devices have also included direct estimations of total corneal astigmatism according to different types of calculations [14-17]. Comparative studies are necessary to evaluate the level of interchangeability of all these measures and how differences among estimations can influence the refractive correction predictability achievable with toric IOLs. The aim of the current study was to compare the keratometric and total corneal astigmatism measures provided by three different technologies as well as to assess the level of interchangeability among them.
2. MATERIALS AND METHODS
2.1. Patients
This prospective comparative study enrolled 94 eyes from 53 patients ranging in age from 29 to 77 years old. All these participants were recruited from the anterior segment consultation at Vithas Eurocanarias Instituto Oftalmológico, where this clinical research was developed. Inclusion criteria were cataract patients or subjects with a transparent crystalline lens but seeking surgical presbyopia correction and being good candidates for lensectomy, aged between 18 and 80 years old, and the possibility of obtaining good quality topographic maps with the three devices. Exclusion criteria were continuous contact lens wear, previous ocular surgery, previous diagnosis of dry eye, corneal opacities or scars, the inability to get good fixation from the patient during corneal topography measurements, and presence of any active ocular or systemic disease. This study was approved by the Ethics Committee of Vithas Eurocanarias and was performed in accordance with the ethical standards laid down in the Declaration of Helsinki. Written informed consent was obtained from all subjects participating in the study.
2.2. Measurement Protocol
The eye examination performed in all eyes included measurement of uncorrected and corrected distance visual acuity, objective and manifest refraction, slit-lamp biomicroscopic examination, Goldmann tonometry, corneal curvature and biometric measurement with the IOL-Master 700 system (Carl Zeiss Meditec AG, Jena, Germany), and corneal topography with the Cassini (i-Optics, The Hague, the Netherlands, distributed by Ophthec) and Pentacam systems (software version 1.14r01, Oculus Optikgeräte GmbH, Wetzlar, Germany). Calibration of both topographers and optical biometer was performed according to the manufacturer’s instructions before initiating the study. All measurements were performed by the same single experienced examiner following the specific sequence IOLMaster-Cassini-Pentacam. Data analysis extraction and analysis were performed by another independent examiner.
The IOL Master 700 is an optical biometer combining the telecentric 3-zone keratometry and swept-source OCT technologies. Besides anatomical measurements, this system provides two corneal parameters, total keratometry (TK) and astigmatism. These parameters are calculated considering anterior and posterior corneal curvature as well as corneal thickness [18]. The Cassini system provides anterior corneal topographic measurements derived from the analysis of the specular reflection of 679 colored light-emitting diodes (LEDs) as well as a measure of the curvature of the posterior corneal surface based on the information obtained from 7 additional projected infrared LEDs [19]. With all this data, the software of the system calculated the total corneal power and astigmatism, including magnitude and axis [19]. Concerning the Pentacam system (Oculus Optikgeräte GmbH, Wetzlar, Germany), it uses Scheimpflug imaging to characterize the anterior segment [20]. A total of 100 images with 500 measurement points are taken with this device on the anterior and posterior corneal surfaces over a 180-degree rotation [20]. Gaussian approaches for the calculation of total corneal astigmatism considering the geometry of both corneal surfaces and pachymetry are provided by this device, such as the calculation of equivalent keratometric readings (EKR) [20].
2.3. Statistical Analysis
Statistical analysis of the results was done using the SPSS program v.19.0.0 for Windows (SPSS Inc., Chicago, IL). According to Kolmogorov–Smirnov test, all studied parameters followed a normal distribution, therefore, parametric tests were applied. Differences between the three devices compared were evaluated for the following parameters: steepest (K2) and flattest standard keratometric readings (K1), steepest (TK2) and flattest total keratometric readings (TK1), and white-to-white corneal diameter (WTW). An analysis of variance (ANOVA) for repeated measures was used to assess the statistical significance of differences. As a post-hoc test, the t-test for paired data, including Bonferroni correction was performed. Pearson correlation coefficients were used to assess the correlation between measures obtained with the three devices evaluated. All statistical tests were 2-tailed, and p-values less than 0.05 were considered statistically significant.
After this, an evaluation of the interchangeability of measurements obtained with the three devices was performed using the Bland-Altman method. The limits of agreement (LoA) were defined as the mean ±1.96 standard deviation (SD) of the differences.
|
IOL-Master 700 (IOLM) |
Cassini (CAS) |
Pentacam (PTC) |
p-value | |
|---|---|---|---|---|
| K1 (D) | 43.13 (1.44) 43.20 (39.14 to 46.36) |
42.74 (1.48) 42.90 (38.90 to 46.14) |
43.02 (1.41) 43.10 (39.00 to 46.10) |
<0.001 IOLM-PTC 0.001 IOLM-CAS <0.001 PTC-CAS <0.001 |
| K2 (D) | 44.01 (1.58) 43.97 (39.66 to 49.01) |
43.69 (1.63) 43.69 (39.14 to 48.46) |
43.90 (1.53) 43.85 (39.40 to 48.80) |
<0.001 IOLM-PTC 0.003 IOLM-CAS <0.001 PTC-CAS <0.001 |
| ΔD_K (D) | 0.88 (0.73) 0.72 (0.00 to 5.26) |
0.95 (0.72) 0.87 (0.05 to 5.15) |
0.88 (0.70) 0.70 (0.00 to 5.10) |
0.007 IOLM-PTC <0.001 IOLM-CAS <0.001 PTC-CAS <0.001 |
| TK1 (D) | 43.19 (1.46) 43.33 (38.99 to 46.54) |
41.68 (1.46) 41.75 (36.21 to 44.80) |
42.86 (1.46) 43.01 (38.45 to 46.01) |
<0.001 IOLM-PTC <0.001 IOLM-CAS <0.001 PTC-CAS <0.001 |
| TK2 (D) | 44.07 (1.57) 44.14 (39.18 to 48.81) |
42.70 (1.57) 42.67 (37.94 to 46.89) |
43.62 (1.52) 43.75 (39.20 to 46.95) |
<0.001 IOLM-PTC <0.001 IOLM-CAS <0.001 PTC-CAS <0.001 |
| ΔD_TK (D) | 0.88 (0.73) 0.67 (0.00 to 5.06) |
1.02 (0.71) 0.87 (0.08 to 4.61) |
0.76 (0.62) 0.65 (0.08 to 4.31) |
<0.001 IOLM-PTC <0.001 IOLM-CAS <0.001 PTC-CAS <0.001 |
| WTW (mm) | 12.05 (0.41) 12.10 (11.20 to 13.00) |
12.38 (0.55) 12.30 (11.30 to 14.70) |
11.64 (0.44) 11.60 (10.50 to 12.80) |
<0.001 IOLM-PTC <0.001 IOLM-CAS <0.001 PTC-CAS <0.001 |
3. RESULTS
The study involved 94 eyes (46 right and 48 left eyes) of 53 subjects (33 males and 61 females) with a mean age of 58.8 years old (range 29 to 77 years). Mean axial length in the analyzed sample was 24.04 ± 1.75 mm (range 21.14 to 28.71 mm) and the mean anterior chamber depth was 3.21 ± 0.41 mm (range 2.27 to 3.99 mm). Mean logMAR CDVA of the eyes evaluated was 0.13 ± 0.19 (range 0.00 to 1.00). Table 1 summarizes the anterior and total corneal topographic parameters obtained with the three topographic devices analyzed. As shown, statistically significant differences were found between devices for all the parameters evaluated (p<0.001). Specifically, standard and total keratometric readings obtained with the IOL-Master system were significantly higher than those obtained with the other two devices (p≤0.003). However, the magnitude of standard and total keratometric astigmatism obtained with the Cassini system was significantly higher than the astigmatic values provided by the other two devices (p<0.001). Likewise, significantly higher values of WTW were obtained with the Cassini system compared to the other two devices (p<0.001).
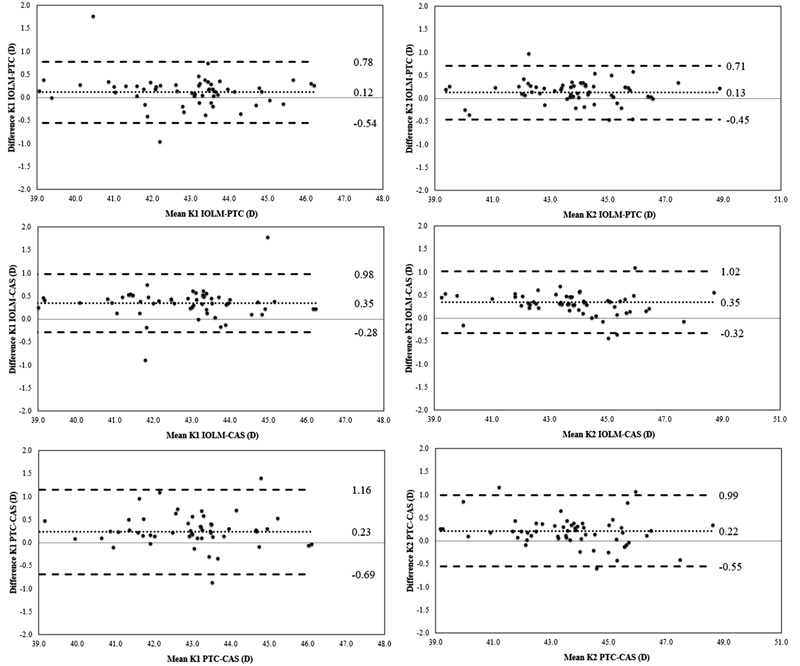
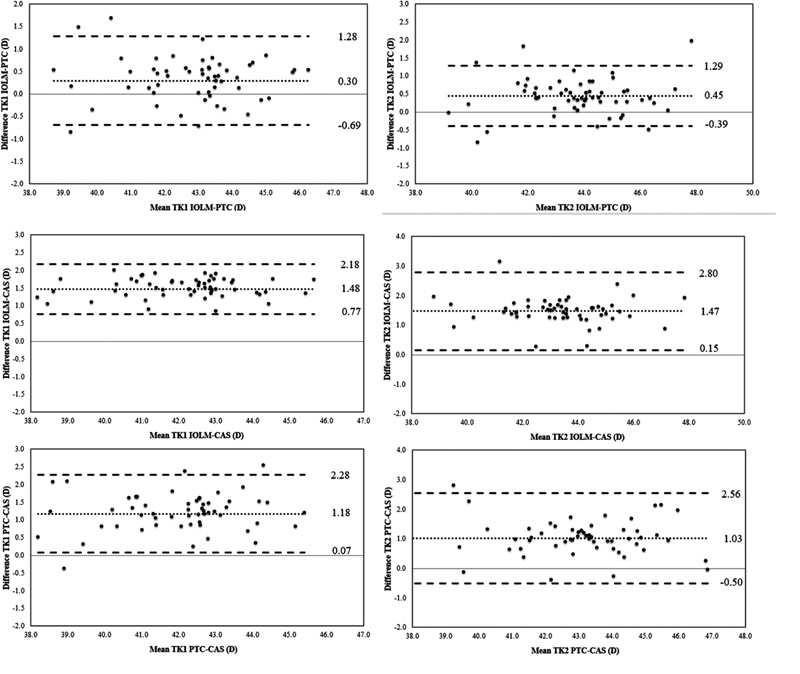
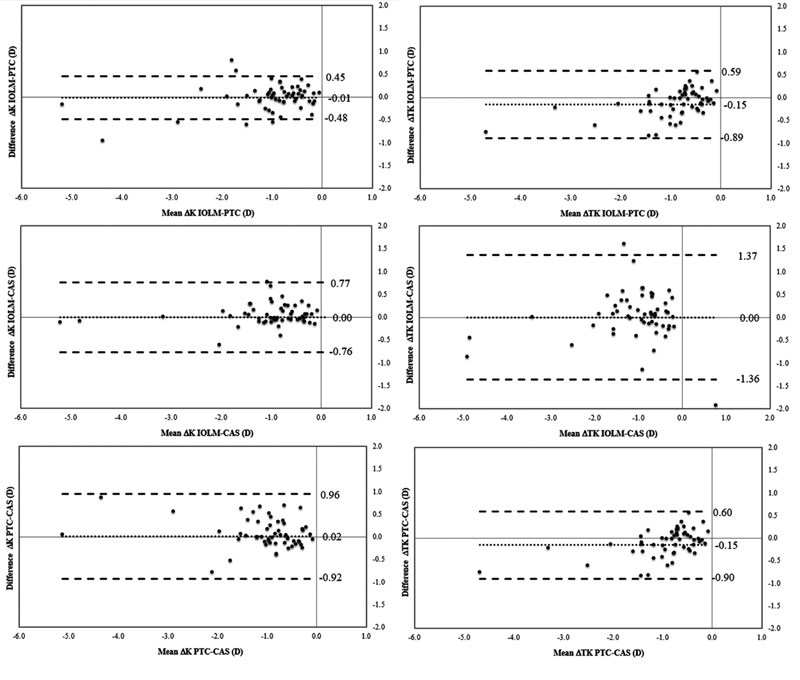
An analysis of the interchangeability of the measures provided by the three devices evaluated was performed using the Bland and Altman method. For standard keratometric readings, ranges of agreement (range from -1.96*SD to 1.96*SD) varied from 0.58 D, for the comparison of K2 obtained with IOL-Master and Pentacam systems, to 1.03 D for the comparison of K1 obtained with Pentacam and Cassini systems (Fig. 1). Concerning total keratometric readings, ranges of agreement varied from 0.70 D, for the comparison of K1 obtained with IOL-Master and Cassini systems, to 1.53 D for the comparison of K2 obtained with Pentacam and Cassini systems (Fig. 2). Ranges of the agreement for standard and total keratometric astigmatism were between 0.46 D, for the comparison of standard keratometric astigmatism obtained with IOL-Master and Pentacam systems, and 1.37 D for the comparison of total keratometric astigmatism obtained with IOL-Master and Cassini systems (Fig. 3)
4. DISCUSSION
The aim of the current study was to analyze the differences between three different commercially available devices in terms of standard and total keratometric measurements, assessing the level of interchangeability between them in eyes with a healthy cornea combined with or without cataract. Specifically, the measurements provided by the IOL-Master 700, Cassini, and Pentacam HD systems have been compared, which are devices that have been shown to provide repeatable measurements of corneal power in healthy eyes [15, 20-24]. The study of these differences is relevant as they can lead to clinically significant inaccuracies in IOL power calculations and consequently, to the presence of unexpected postoperative residual refractive errors after cataract surgery. A 0.5-D difference in the corneal plane induces a difference of more than 0.5 D (about 0.73 D) in the IOL plane [25].
4.1. Comparison of Standard Keratometric Measures of the Three Devices
Significantly higher values of standard keratometric readings were obtained with the IOL-Master compared to the other two devices. These differences were also clinically relevant, with ranges of agreement between devices over 0.50 D. Therefore, the keratometric readings provided by these three devices cannot be used as interchangeable. This is consistent with the results of a previous comparative study of keratometric measurements provided by the IOL-Master 500, Cassini, and Pentacam systems [26]. These authors confirmed that the previous model of the IOL-Master system (500) provided steeper curvature measurements, compatible with higher corneal power values, as compared to Cassini and Pentacam systems in healthy eyes [26]. Muzyka-Wozniak et al. [27] also found flatter curvature values with the Pentacam system in comparison with IOL-Master, as well as other authors in other comparative studies [28-30]. However, Hidalgo and colleagues [23] obtained steeper central curvatures with the Cassini system compared to values obtained with a Placido-based system and the Scheimpflug based device Pentacam HR. Several factors may account for the clinically relevant differences in standard keratometry between devices, with the area of analysis used for the calculation of keratometric measurements being one of them. It should be considered that keratometry is calculated for a 3-mm area with the Pentacam and Cassini topography systems, whereas calculations with the IOL-Master system are performed for a 2.5-mm optical zone. Likewise, the use of different mathematical approaches for the keratometric estimation may explain these statistically and clinically significant differences between devices.
4.2. Comparison of Total Keratometric Measures of the Three Devices
As happened with standard keratometry, significantly higher values of total keratometric readings were obtained with the IOL-Master compared to Cassini and Pentacam systems. This is consistent with the results of previous comparative studies of Cassini and Scheimpflug imaging-based topographers, confirming the presence of statistically significant differences in total corneal power among these two technologies [16, 31, 32]. Besides differences in the algorithms used for the calculation of total power among devices, the main factor contributing to discrepancies in total corneal power seems to be the different measures of posterior corneal curvature provided by each device evaluated. A trend of the Cassini system of obtaining flatter posterior corneal curvature measurements compared to those provided by the Pentacam system has been consistently reported [22]. More research is still needed to understand and find the exact reason for this relevant discrepancy in posterior corneal curvature measurements between color light-emitting diode and Scheimpflug imaging technologies.
4.3. Comparison of Standard and Total Corneal Astigmatism Measures of the Three Devices
Finally, statistically significant differences among devices have also been found in the magnitude of standard and total keratometric astigmatism, with the highest values provided by the Cassini system. Likewise, these differences have also been found to be clinically relevant, with ranges of agreement between measurement systems over 0.45 D. This contrasts with the previous series showing no clinically relevant differences in anterior corneal astigmatism between Cassini and Pentacam systems [15, 16, 23]. Another comparative study between IOL-Master 500, Cassini, and Pentacam detected differences in the limit of statistical significance among devices for anterior keratometric astigmatism measures, but they were clinically relevant according to the Bland-Altman analysis [26]. Concerning total keratometric astigmatism measurements, differences among Pentacam and Cassini systems were found to be statistically significant as well as clinically relevant [15, 16, 26]. This suggests that one of the critical factors leading to relevant differences in the calculation of total corneal astigmatism among Pentacam and Cassini is the different modes of both technologies of characterizing the posterior corneal shape. In any case, the use of different mathematical approaches with each device evaluated for calculating the combined effect of anterior and posterior corneal optical surfaces can also have a very relevant influence on astigmatic discrepancies between devices. These differences should be considered in clinical practice when using total corneal power and astigmatism measures for a different purpose, such as IOL power calculations.
CONCLUSION
In conclusion, standard and total keratometric readings and astigmatism measures obtained with IOL-Master 700, Cassini, and Pentacam systems cannot be used interchangeably, as there are statistically significant and clinically relevant differences among devices. Therefore, if the data of these three systems are used for toric IOL power calculations, significant differences can be expected. Specifically, the IOL-Master 700 system provides higher corneal power measurements than the other two devices, whereas the Cassini topographer provides a higher magnitude of anterior and total corneal astigmatism. Future studies should be conducted to characterize the impact of the differences in the estimation of corneal power and astigmatism among devices on the refractive predictability achieved with different toric IOLs. This type of study would allow defining the best corneal evaluation approach for optimizing toric IOL power calculations.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethics Committee of Vithas Eurocanarias, Alicante, Spain under approval no. (CASSINI-19-01).
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all individual participants included in the study.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
The author, David P Piñero, has been supported by the Ministry of Economy, Industry, and Competitiveness of Spain within the program Ramón y Cajal, RYC-2016-20471.
CONFLICTS OF INTEREST
The authors have no proprietary or commercial interest in the medical devices that are involved in this manuscript.
ACKNOWLEDGEMENTS
Declared None.

