All published articles of this journal are available on ScienceDirect.

Refractive, Visual and Retinal Outcomes after Intravitreal Ranibizumab Monotherapy for Retinopathy of Prematurity
Authors Info & Affiliations
Abstract
Background:
Intravitreal ranibizumab (IVR) is increasingly used as an off-label treatment for retinopathy of prematurity (ROP). The most clinically used dose is 0.25 mg; however, its late outcomes are rarely reported. This study compares the late refractive, visual, and retinal outcomes in children with type 1 ROP treated with 0.25 mg IVR to those with type 2 ROP that regressed spontaneously.
Methods:
This retrospective study included 48 children (96 eyes) with ROP history. Birth history data, spherical equivalent (SE) of cycloplegic refraction, and the prevalence of visual and retinal anomalies were compared between type 1 (68 eyes) and type 2 ROP (28 eyes).
Results:
At a mean age of 3.47 years, children with type 1 ROP had significantly lower mean SE (+0.17D ± 3.60) than children with type 2 ROP (+1.99D ± 2.80) (P = 0.02). SE was significantly affected by repeated injections of IVR, leading to a reduction of SE and myopic shift. Risk factors of high myopia (SE ≤ -5 diopters) include the presence of respiratory distress syndrome (RDS) (P = 0.01), advanced maternal age (P=0.02), in vitro fertilization (IVF) (P = 0.02), ROP type 1 (P = 0.01) ROP in zone 1 (P = 0.01) and repeated IVR treatment (P= 0.01). No significant difference was found between ROP types in the prevalence of hyperopia, myopia or emmetropia. The prevalence of visual anomalies (strabismus, fixation anomalies, nystagmus, amblyopia, and extraocular imbalances) and retinal anomalies (anomalies of the retinal surface, vasculature, and optic disc) were not significantly different between the groups.
Conclusion:
IVR monotherapy with 0.25 mg for ROP resulted in the myopic shift. Repeated IVR treatment increases the risk of high myopia. High myopia is also significantly associated with RDS, IVF, advanced maternal age, type 1 ROP, and ROP in zone 1. No association was found between IVR and visual or retinal anomalies.
1. INTRODUCTION
Retinopathy of prematurity (ROP) is a proliferative vascular disease affecting the developing retinal vessels of premature infants, which is considered a leading cause of childhood blindness worldwide [1]. It is estimated that ROP is the cause of blindness of more than 20000 children and the visual impairment of additional 12300 children every year [2]. The key risk factors associated with ROP development include early gestational age [3], prolonged oxygen exposure [4, 5] and low birth weight [6].
In a premature hypoxic retina, vascular endothelial growth factors (VEGFs) stimulate the growth of new, abnormal blood vessels that compensate for tissue ischemia, hence contributing to the development of ROP [7]. In recent years, intravitreal anti-VEGF therapy has been introduced as a treatment modality for ROP, it has been attracting a lot of attention due to its non-destructive mechanism that permits normal development of the peripheral retinal vasculature, allowing for uncompromised visual field [8].
Ranibizumab (Lucentis) is a humanized 49-kilodalton monoclonal antibody fragment that is active against all isoforms of VEGF. It was approved for intravitreal use by the FDA in 2006 [9]. It is characterized by small molecular size, which grants intravitreal injection two advantages; the first is better tissue penetration, and the second is a short systemic half-life. Therefore, IVR has been favored over other anti-VEGF drugs in cases where systemic side effects are of concern. However, a possible drawback of the short half-life of IVR is the risk of ROP recurrence, compared with other anti-VEGF drugs [10, 11].
The most commonly used dose of IVR is 0.25 mg, as it is half the dose used in adults. However, not many studies reported the late outcome of this dose. A Chinese study by Meng et al. aimed to investigate the refractive outcomes of this dose after 2 years of treatment and reported a high prevalence of myopia, up to 37% [12]. Another study in Turkey compared the outcomes of different treatment modalities for type 1 ROP, including intravitreal bevacizumab, ranibizumab and laser photocoagulation, and reported that all groups demonstrated myopic refractive error [13]. A more recent study also compared the outcomes of IVR with laser photocoagulation, which reported no significant difference in the prevalence of myopia and anisometropia between the groups, yet, strabismus was more common in the laser group [14]. To our knowledge, no study in the literature has compared the outcomes of 0.25 mg of IVR for type 1 ROP treatment with the outcomes in eyes with type 2 ROP that regressed spontaneously, which we think will provide valuable insights on the influence of this dose on the development of premature eyes.
This study compares the refractive, visual, and retinal outcomes in eyes treated with 0.25 mg of IVR for type 1 ROP with the outcomes in eyes with type 2 ROP. Moreover, this study aims to find the factors that play a role in refractive outcomes, including disease-related factors, such as ROP severity and recurrence, as well as maternal and neonatal factors. In addition, this study aims to report the prevalence of visual anomalies, including amblyopia, strabismus, nystagmus and fixation anomalies in the eye treated with 0.25 mg of IVR compared with eyes with type 2 ROP, which will provide knowledge on the impact of this dose on development of ocular structures.
2. MATERIALS AND METHODS
This is a retrospective study conducted at King Abdullah Children's Specialist Hospital in Riyadh, Saudi Arabia. The Institutional Review Board of King Abdullah International Medical Research Center (KAIMRC) approved the study. The study population included all children born from 2015 to 2019 with a history of ROP. The subjects were divided into 2 groups based on Early Treatment for Retinopathy of Prematurity (ETROP) criteria into type 1 ROP and type 2 ROP [15]. Type 1 ROP group included all children requiring treatment who received at least one injection of 0.25 mg ranibizumab (Lucentis ®). Type 2 ROP group included all children who had spontaneously regressed ROP and received no ranibizumab treatment or any other treatment.
Data collection started from September to November of 2021. Data were obtained from hospital medical records, including stage, and zone of ROP in each eye, presence of plus disease, presence of aggressive ROP (A-ROP) [16], age at treatment, frequency of ROP reactivations, the total number of IVR injections, and duration of complete regression of ROP.
Moreover, the late outcomes of treatment were recorded, including refractive, visual, and retinal findings. The refractive findings include the spherical equivalent (SE) of cycloplegic refraction with the retinoscope. Based on the mean SE of cycloplegic refraction, the study population was classified into: Myopes (SE ≤ −0.5 D), emmetropes (SE > −0.25 D to +0.25 D), and hyperopes (SE > +0.50 D). High myopia was defined as SE of ≤ −5.00 D. The visual findings include data regarding orthoptic status, the pattern of fixation, and extraocular muscles balance assessment, with the evaluation of the presence of amblyopia, strabismus, and nystagmus. Furthermore, visual acuity was obtained for the children who were able to complete the visual acuity examination. The retinal findings include the evaluation of retinal vasculature, retinal surface, and optic disc in each eye. The retinal assessment was done primarily by a single experienced ophthalmologist who documented the retinal findings. Retinal vasculature is defined as normal when there are no detectable avascular areas, retinal thinning, fibrosis, abnormal tortuosity, or any other vascular anomaly. The retinal surface is considered normal when the surface appears healthy with no signs of retinal detachment, macular or retinal scars or any other abnormality. The optic disc is defined as normal in the case of the absence of disc pallor and abnormal disc shape or appearance.
Data regarding birth history were also recorded, including birth weight, gestational age, route of delivery, presence of respiratory distress syndrome, multiple pregnancies, use of in vitro fertilization and maternal age. Additionally, the presence of developmental delay was documented.
Data were analyzed using SAS software (SAS Institute Inc, Cary, NC) version 9.4. Fisher’s Exact and chi-square tests were used to compare qualitative data. Quantitative data were analyzed using Wilcoxon two-sample test and the Kruskal-Wallis test. Pearson correlation (R2) was used to assess various inter-eye correlations. Multiple linear regression test was used to determine factors affecting SE, development of high myopia, and ROP recurrence. The level of significance was determined at P ≤ 0.05.
3. RESULTS
3.1. Demographic Data
A total of 96 eyes of 48 children were included in this study. The mean GA was 25.33 ± 2.80 weeks, with 56.25% males and 43.75% females. The mean BW was 778.96 ± 329.52 grams; the median was 710 grams (ranging from a minimum of 500 grams to a maximum of 2100 grams). Type 1 ROP group included a total of 68 eyes of 34 children (70.83%), while type 2 ROP group included 28 eyes of 14 children (29.17%). High correlation was found between the right and left eyes regarding the ROP stage (R2 = 0.94) and ROP zone (R2 = 0.77). Table 1 demonstrates the demographic data and clinical characteristics of children with type 1 and type 2 ROP.
There were no significant differences in gender, route of delivery, the prevalence of multiple pregnancies, presence of respiratory distress syndrome, the use of in vitro fertilization, maternal age, and the presence of developmental delay between type 1 and type 2 ROP. A significant difference was found between ROP types in birth weight (P=0.01), gestational age (P=0.01), and regression duration (P=0.01). One of the children was diagnosed with the Plus disease in both eyes. No zone was specified for either eye. The delivery route of 2 children with type 1 ROP could not be verified due to missing data.
3.2. Refractive Outcomes
One child had a non-functional eye, in which the cycloplegic refraction was not performed, for all other 95 eyes, the cycloplegic refraction was recorded. Children were examined at a mean age of 3.47± 1.27 years, there was no significant difference in the mean age at examination between the type 1 ROP group and type 1 (P=0.06). The prevalence of different types of refractive error and the mean SE are demonstrated in Table 2.
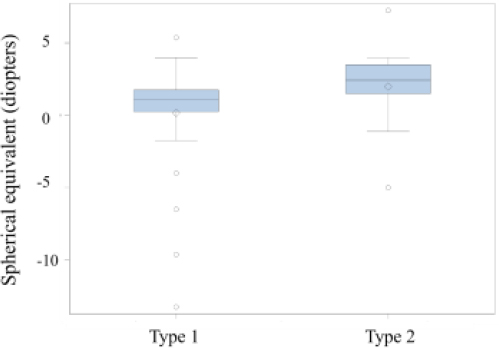
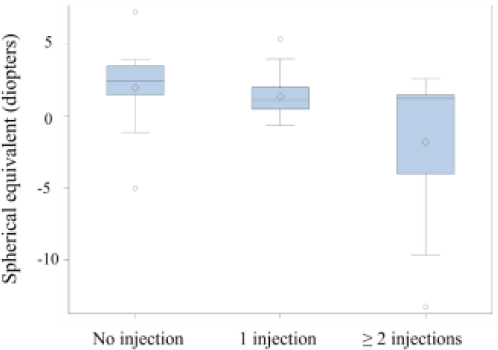
There was a high correlation in the SE between the right and left eyes, with an R2 coefficient of 0.79. The distribution of hyperopia, myopia and emmetropia was not significantly different between type 1 & 2 ROP. However, hyperopia was the most common type of refraction in both groups, followed by myopia, then emmetropia. The mean SE was significantly lower in type 1 than in type 2, although both were within the hyperopic range (Fig. 1). Using multiple linear regression tests, we found that the number of administrated IVR injections significantly influenced the mean SE, as repeated injections resulted in a significant reduction of SE and myopic shift (P < 0.05), as shown in Fig. (2).
Multiple linear regression tests revealed that the risk of high myopia (SE ≤ -5 diopters) is significantly influenced by the presence of RDS (P = 0.01), maternal age (P=0.02), IVF (P = 0.02), ROP type (P = 0.01) ROP zone (P = 0.01) and number of IVR injections (P= 0.01). Table 3 demonstrates the association between the number of injections with the mean SE and the prevalence of high myopia.
| - | Type 1 ROP | Type 2 ROP | P | |
| Gender (M/F) (N%) | 20 (58.82%)/ 14(41.18%) | 7(50%), 7(50%) | 0.75 | |
| Mean GA (weeks) | 24.26 ± 1.60 | 27.07 ± 4.16 | *0.01 | |
| Mean BW (grams) | 661.63 ± 158.16 | 1047. 14 ± 452.63 | *0.01 | |
| ROP zone | Zone 1 n (%)Zone 2 n (%)Zone 3 n (%) | 6 (17.65%) 27 (79.41%)0 | 012 (85.71%)2 (14.28%) | *0.04 |
| ROP stage | Stage 1 n (%)Stage 2 n (%)Stage 3 n (%)A-ROP n (%) | 0026 (76.47%)8 (23.53%) | 5 (35.71%)8 (57.41%)1 (7.14%)0 | *0.01 |
| Plus disease (%) | 33 (97.06%) | 0 | *<0.01 | |
| Delivery route (Normal spontaneous delivery/C-section) (%) | 20 (62.50%)/ 12 (37.50%) | 10 (71.43%)/ 4 (28.57%) | 0.74 | |
| Multiple pregnancy % | 43.75% | 14.29% | 0.24 | |
| Respiratory distress syndrome n (%) | 27 (90%) | 11 (78.57%) | 0.36 | |
| In vitro fertilization n (%) | 7 (22.58%) | 0 | 0.08 | |
| Maternal age (years) | 30.00 ± 6.52 | 30.23 ± 6.15 | 0.95 | |
| Developmental delay n (%) | 7 (21.88%) | 2 (14.29%) | 0.70 | |
| Mean regression duration (months) | 4.17 ± 2.01 | 1.58 ± 1.00 | *0.01 | |
| - | Type 1 ROP | Type 2 ROP | P |
|---|---|---|---|
| Hyperopic eyes n (%) | 51 (76.12%) | 22 (78.57%) | 0.80 |
| Myopic eyes n (%) | 13 (19.40%) | 5 (17.86%) | 0.86 |
| Emmetropic eyes n (%) | 3 (4.48%) | 1 (3.57%) | 0.84 |
| Mean SE | 0.17 D ± 3.60 | 1.99 D ± 2.80 | *0.02 |
| - | No Injection(28 eyes) | 1 Injection(42 eyes) | 2+ Injections(26 eyes) | P |
|---|---|---|---|---|
| Mean SE | +1.99 D ± 2.80 | +1.38 D ± 1.39 | -1.79 ± 5.07 | *0.02 |
| High myopia n (%) | 1 eye (3.57%) | 0 | 7 eyes (26.92%) | *0.01 |
| - | Type 1 ROP | Type 2 ROP | P |
|---|---|---|---|
| Strabismus (%) | 12 (35.29%) | 6 (42.86%) | 0.75 |
| Nystagmus (%) | 4 (14.76%) | 0.00 | 0.31 |
| Fixation anomalies (%) | 4 (11.76%) | 2 (14.17%) | >0.58 |
| Amblyopia (%) | 6 (17.65%) | 4 (28.57%) | 0.45 |
| Extraocular muscle anomalies (%) | 0.00 | 2 (14.29%) | 0.08 |
| - | Type 1 ROP | Type 2 ROP | P |
|---|---|---|---|
| Normal Retinal Vasculature (eyes %) | 75% | 100% | >0.29 |
| Avascular zone 3/ avascular zone 2 & 3Generalized thinningIncreased vascular tortuosityFibrous retina | 1.47%/ 2.94%2.94%2.94%1.47% | - | - |
| Normal Retinal Surface (eyes %) | 95.59% | 100% | 1.00 |
| Retinal detachmentRPE changed with macular scar*Photocoagulation | 1.47%1.47%1.47% | - | - |
| Normal Optic Disc (eyes %) | 85.3% | 92.86% | >0.40 |
| Disc pallorTilted discTemporal disc dragging | 11.76%1.47%1.47% | 7.14% | - |
3.3. Visual Outcomes
The prevalence of strabismus, nystagmus, fixation anomalies, amblyopia and extraocular anomalies were evaluated and compared between type 1 and type 2 ROP groups, and no significant difference was found (Table 4).
The type 2 ROP group demonstrated a higher prevalence of strabismus, fixation anomalies, amblyopia, and extraocular anomalies. However, the difference was not statistically significant. Nystagmus was limited to the type 1 ROP group as no child with the type 2 ROP group had nystagmus, yet the difference was not statistically significant.
Visual acuity examination was completed for 24 eyes, all of whom could attain the vision of 20/50 or better. 22 eyes with type 1 ROP achieved visual acuity of 20/40 or better, 2 eyes with type 2 ROP achieved 20/40 and 20/50 visual acuity.
3.4. Retinal Outcomes and Reactivation
The retinal findings in the right eyes were highly correlated with the findings in the left eyes, including the appearance of retinal vasculature (R2 = 0.70) and optic disc findings (R2 = 0.53). The retinal findings were evaluated and compared between type 1 and type 2, as summarized in Table 5. Type 2 ROP group demonstrated a higher prevalence of normal retinal findings than the type 1 ROP group, including normal retinal vasculature, normal retinal surface, and optic disc. However, the difference was not statistically significant.
Children received the first intravitreal ranibizumab injection at a mean postmenstrual age of 36.19±2.90 weeks. All children diagnosed with type 1 ROP were followed up every week to monitor the progression of the disease. Reactivation of ROP occurred in 13 children (27.08%), 10 children received 2 injections per eye and 3 children received more than 2 injections per eye. Reactivation of ROP occurred in 8 eyes with zone 1 ROP and 16 eyes with zone 2 ROP during the postmenstrual age of 38.86 weeks to 52 weeks. The linear regression test revealed a significant association between type 1 ROP and recurrence of ROP.
4. DISCUSSION
In the past decade, anti-VEGF therapy has been implemented as a primary monotherapy for ROP. Ranibizumab has proven its efficacy in rapid disease regression, promoting the extension of normal vasculature into the peripheral retina [17-19].
This study showed that the majority of eyes treated with 0.25 mg of ranibizumab achieved good anatomical retinal outcomes with almost full vascularization, this is confident with the majority of studies in the literature [13, 17, 20, 21]. Recurrence after IVR treatment is largely variable in the literature, ranging from 13.6% to 83% [22-24], which is mainly due to variation in sample size and dose concentrations. In our study, 27% of eyes needed retreatment, which occurred during the postmenstrual age of 38.86 weeks to 52 weeks. It has been reported that ROP can be reactivated after anti-VEGF therapy at an older postmenstrual age of 69 weeks [25]; thus, it is crucial to keep extended follow-up examinations to confirm complete regression of the disease. In our study, children with type 2 ROP achieved complete regression in significantly shorter duration compared with children with type 1 ROP. This can be explained by the recurrence rate in type 1, as these children were observed for a prolonged period to exclude the risk of recurrence.
Regarding the refractive outcomes, our results showed a negative correlation between the number of injections and the spherical equivalent, as we appraised that repeated injections of 0.25 mg IVR are associated with a reduction in mean SE. Eyes treated with a single dose of IVR had lower mean SE than eyes that did not receive ranibizumab treatment. However, the mean SE was still within the hyperopic range after a single IVR injection. This finding is compatible with other studies which reported that IVR resulted in a myopic shift in refraction al [13, 26].
Chen et al. [26] and Kabataş et al. [13] reported similar findings in which IVR resulted in a myopic shift in refraction. However, they reported myopia to be more prevalent in eyes treated with a single dose of ranibizumab, while we found hyperopia to be the dominant type of refraction despite the myopic shift. The current finding could be attributed to the difference in sample size, as 42 eyes received one injection of ranibizumab compared to 10 and 26 in Kabatas’s [13] and Chen’s studies [26], respectively.
Our results disclosed that eyes that have received several injections of ranibizumab had dominant myopic refraction, with a significant prevalence of high myopia. In our study, 10.29% of eyes in type 1 ROP had high myopia, all of which received multiple IVR injections. This agrees with the findings of Meng et al. [12], where found high myopia to be associated with IVR retreatment. This finding indicates that intravitreal ranibizumab promotes myopic refractive shift. Development of myopia could be attributed to the severity of the disease, which may require retreatment and adverse outcomes, combined with the alterations of VEGF levels in the retina associated with loss of retinal neural cells [27].
This study revealed several risk factors that have a significant association with myopia development; factors related to the nature of the disease, including type 1 ROP, presence of ROP in zone 1 and repeated treatment with IVR. In addition to factors associated with maternal and birth history, including the presence of RDS, IVF conception and older maternal age. Previous studies have initiated a relationship between these factors and the development of ROP [28], but we also found that they play a role in the refractive outcome.
We did not observe significant unfavorable visual outcomes in eyes treated with ranibizumab, we found a higher prevalence of strabismus, amblyopia, and extraocular muscle anomalies in type 2 ROP compared with type 1 ROP, indicating that IVR is not associated with adverse visual outcomes. Stahl and colleagues used ranibizumab in lower concentrations than used in our study (0.12 mg and 0.20 mg), and they reported a higher prevalence of strabismus (44%), nystagmus (31%), and anomalies of motility (12%) compared with our findings (35.29%, 11.67% 0%, respectively) [29]. The different findings could be attributed to differences in dose concentrations in addition to differences in sample size.
We established a non-significant correlation between ranibizumab and the occurrence of developmental delay, even after repetitive injections. This indicates that ranibizumab does not interfere with systemic VEGF in a way that impacts development. This may be due to the short half-life of ranibizumab compared with other anti-VEGF agents. In our study, the developmental delay was present in 21.88% of children treated with ranibizumab, compared with 14.29% in the children who received no treatment; the difference was not statistically significant. This assuring finding suggests that developmental delay is not a result of anti-VEGF therapy but could be attributed to prematurity. In a recent study conducted in 15 regions in 10 European countries, the prevalence of developmental impairment in infants with gestational age less than 32 weeks was 17.3%. In our study, the mean GA of children in type 1 ROP was 24.62 weeks, which is classified as extreme maturity that is associated with numerous morbidities, including developmental delay [30].
Due to the retrospective nature of this study, a limitation of missing data was encountered during the data collection process. Visual acuity was not recorded in most children; this is due to the young age of the children, along with the presence of developmental delay in some children. Additionally, the study was limited by a small sample size. Further longitudinal studies with more subjects and prospective nature are recommended to investigate the visual outcomes more thoroughly.
CONCLUSION
In conclusion, based on the results of the current study, we found 0.25 mg of intravitreal ranibizumab is an effective treatment in ROP, with substantially good anatomical outcomes that achieved peripheral retinal vascularization in most eyes. The visual outcomes are mostly favorable, with a mild reduction in SE after a single injection of 0.25 mg ranibizumab. However, eyes treated with several ranibizumab injections are at risk of developing high myopia. Also, the presence of RDS, type 1 ROP, ROP in zone 1, IVF conception and advanced maternal age are associated with the development of high myopia. To the best of our knowledge, our study is unique in the literature in comparing the refractive outcomes between type 1 & 2 ROP, which provides useful information about the safety and consequences of this dose on premature eyes.
AUTHORS’ CONTRIBUTION
NHA and RMF designed the study, NHA and FA collected the data, and the manuscript was written by NHA and revised by RMF, AA and MH. MA, AA and OA did data analysis, MH contributed to obtaining the study approval, and the study was supervised by RMF.
LIST OF ABBREVIATIONS
| A-ROP | = Aggressive Retinopathy of Prematurity |
| BW | = Birth Weight |
| D | = Diopter |
| FDA | = Food and Drug Administration |
| GA | = Gestational Age |
| IVF | = In vitro Fertilization |
| IVR | = Intravitreal Ranibizumab |
| Mg | = Milligram |
| PMA | = Postmenstrual Age |
| RDS | = Respiratory Distress Syndrome |
| ROP | = Retinopathy of Prematurity |
| SE | = Spherical Equivalent |
| VEGF | = Vascular Endothelial Growth Factors |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Institutional Review Board of King Abdullah International Medical Research Center (KAIMRC) with the given study number SP21R/023/02.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Patient consent was waived due to the retrospective nature of the data and the anonymous use of data.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The datasets used and analyzed during the current study are available from the corresponding author [N.H.A] upon reasonable request.
FUNDING
No funds were received for this study from any organization.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
ACKNOWLEDGMENTS
Special thanks to King Saud University and King Abdullah Children Specialist Hospital in Riyadh for helping in conducting this study.

