All published articles of this journal are available on ScienceDirect.

Comprehensive Visual Acuity Outcomes after EDOF versus Enhanced Monofocal IOL Implantation in Indian Cataract Patients
Abstract
Introduction
The study compared visual acuity and refractive outcomes of EyecrylTM SERT and TECNIS Eyhance™ IOLs following cataract surgery as part of a broader prospective evaluation.
Methods
This is a prospective, non-randomized comparative study of cataract patients implanted with either IOL. Postoperative assessments were conducted at Day 1, Week 2, and Month 6. Outcomes included corrected and uncorrected distance, near, and intermediate visual acuity, intraocular pressure, and refractive parameters.
Results
The study included 120 eyes (60 per group). At 6 months, Eyecryl™ SERT demonstrated better monocular and binocular DCIVA than TECNIS Eyhance™ (0.10 ± 0.08 vs. 0.15 ± 0.08 logMAR; p < 0.0001 and 0.07 ± 0.06 vs. 0.11 ± 0.09 logMAR; p = 0.0021, respectively). Binocular UCIVA also favored Eyecryl™ SERT (0.09 ± 0.08 vs. 0.16 ± 0.09 logMAR; p = 0.0005), while monocular UCIVA was comparable between groups. Both groups showed significant improvement in monocular UDVA and BCDVA from baseline, with no significant inter-group differences. Binocular UDVA and BCDVA remained stable in both groups, with no significant intra- or inter-group differences. TECNIS Eyhance™ showed significantly better monocular and binocular UNVA and better binocular DCNVA, whereas monocular DCNVA was comparable between groups. IOP remained within normal limits, and refractive parameters were comparable between groups.
Discussion
Visual acuity assessment across multiple distances under monocular and binocular conditions helped identify optical trade-offs and suitability for visual rehabilitation.
Conclusion
Eyecryl™ SERT demonstrated better intermediate vision compared to TECNIS Eyhance™ following cataract surgery, with both lenses showing favorable safety profiles over 6 months.
1. INTRODUCTION
Presbyopia is an inevitable age-related condition, currently affecting nearly one billion people worldwide [1]. With the advent of monofocal Intraocular Lenses (IOLs), significant research has focused on addressing the loss of accommodation, leading to the development of advanced lens designs such as multifocal IOLs. From an optical standpoint, multifocal IOLs use diffractive or refractive optics to create additional focal points, helping patients achieve clearer near and intermediate vision. Although they enhance spectacle independence, these lenses can sometimes cause visual disturbances such as halos, glare, and starbursts, especially in low-light conditions [2, 3]. Depending on the number of functional foci, these lenses can be categorized as bifocal or trifocal.
To overcome these limitations, accommodative IOLs were designed in the early 2000s to mimic physiological accommodation through anterior-posterior movement or changes in lens shape and have shown variable long-term outcomes. [4] Their performance is frequently affected by posterior capsular Opacification (PCO), capsular contraction, and lens tilt, which can result in asymmetric vaulting and unstable refractive outcomes. As a result, accommodative IOLs have become less favored in routine clinical practice due to limitations in both efficacy and predictability [4, 5].
In contrast, Extended Depth of Focus (EDOF) IOLs have emerged as a promising alternative, offering various advantages over both multifocal and accommodative lenses. Designed in the mid-2010s, they create a single elongated focal point, extending the range of clear vision from distance to intermediate distances without generating multiple distinct focal points. This optical strategy minimizes the overlap of in-focus and out-of-focus images, thereby reducing dysphotopsia and preserving contrast sensitivity [6]. The EyecrylTM SERT IOL (Biotech Vision Care Pvt. Ltd.) is a hydrophobic Aspheric EDOF IOL with an aspheric surface that leverages proprietary Monomore® technology, which features optimized optical zones for extended vision, asymmetric power distribution to reduce pupil dependency, and maintains low levels of Photic phenomena, similar to standard monofocal IOLs. [7] The TECNIS SIMPLICITY™ Delivery System Model DIB00 (Johnson & Johnson Vision) contains the TECNIS Eyhance™ IOL; on the other hand, it is a one-piece, foldable, posterior chamber lens whose optical designs are associated with a certain amount of depth of focus. The TECNIS Eyhance™ IOL is designed to slightly extend the depth of focus compared to the monofocal analogue TECNIS™ 1-Piece IOL, Model ZCB00. [8].
The current study is part of a large, prospective, non-randomized clinical study aimed at evaluating the performance and safety of the EyecrylTM SERT and TECNIS Eyhance™ IOLs and is solely focused on comparing various visual acuities and refractive outcomes associated with these IOLs following cataract surgery.
2. METHODS
2.1. Study Design and Patients
This prospective, non-randomized comparative clinical study was conducted at Nethradhama Super Specialty Eye Hospital, Bangalore, Karnataka, India, following approval from Nethradhama Super Specialty Eye Hospital, Institutional Ethical Committee (IEC/IRB No. 2022/12). All the surgeries were performed between August 2022 and May 2024. The study adhered to the principles outlined in the Declaration of Helsinki. Patients were enrolled consecutively in a prospective manner, and lens selection reflected routine clinical practice and availability during the study period. Written informed consent was obtained from all participants after providing a detailed explanation of the study protocol. The trial was prospectively registered with the Clinical Trials Registry of India (CTRI/2022/05/042838). This study represents a secondary analysis of data obtained from a larger prospective investigation of two intraocular lenses, with the current report specifically focusing on various visual acuities and related refractive outcomes.
The study enrolled cataract patients aged ≥22 years with a preoperative BCDVA of 20/40 or worse, an anticipated postoperative BCDVA better than 20/30, and keratometric astigmatism ≤0.75 D. Patients were excluded if they had systemic illness or medications increasing surgical risk, ocular conditions predisposing to complications, prior corneal or intraocular surgery, degenerative retinal or macular disorders, or factors affecting IOL centration. Pregnant or lactating women, individuals with hormonally related refractive fluctuations, and those requiring retinal laser procedures with a risk of light scatter were also excluded.
2.2. Preoperative Examination
Patients underwent a full ophthalmic evaluation, including ETDRS (Precision Vision) -based visual acuity testing, slit-lamp and dilated fundus examination, and IOP measurement with Goldmann applanation tonometry. IOL power was determined using the IOL Master 700 biometer with the Barrett Universal II formula.
2.3. Study IOLs
The EyecrylTM SERT is a preloaded, single-piece, foldable hydrophobic acrylic posterior chamber IOL (<5% water content) designed to replace the natural crystalline lens. The TECNIS Eyhance™ IOL (Model DIB00) with the Simplicity™ Delivery System is an ultraviolet-light- absorbing posterior chamber lens implanted in the capsular bag to restore optical function (Table 1).
| No. | Parameters | Description | |
|---|---|---|---|
| EyecrylTM SERT IOL | TECNIS Eyhance™ IOL | ||
| 1. | Material | Hydrophobic Acrylic containing natural chromophore | soft foldable hydrophobic acrylic c with a covalently bound UV absorber |
| 2. | Optic Type | Single piece, 360-degree square edge with refractive aspheric optic | 1-Piece IOL, ProTEC frosted, continuous 360° posterior square edge |
| 3. | Optics diameter | 6.00 mm | 6.00 mm |
| 4. | Overall diameter | 13.00mm | 13.0 mm |
| 5. | Refractive index | 1.524 | 1.47 at 35° C |
| 6. | Diopter range | +7.0D to +30.0D (with 0.5D step) | +5.0 D to +34.0 D in 0.5 diopter increments |
| 7. | Delivery system | Pre-loaded delivery system | Tecnis Simplicity system |
2.4. Surgical Procedure
All surgeries were performed by a single surgeon (SG) under 0.5% proparacaine and intracameral 2% lidocaine eyedrops. A 2.8-mm temporal biplanar incision was created, and phacoemulsification was carried out using the Centurion® Vision System (Alcon). Continuous curvilinear capsulorhexis (5.0-5.5 mm) was performed manually with a 26G cystitome or femtosecond laser. Standard preoperative mydriatics (tropicamide 0.5% with phenylephrine hydrochloride) and anti-inflammatory drops (flurbiprofen 0.1%) were used. Aurovisc (Aurolab) served as the viscoelastic agent to maintain chamber stability and facilitate IOL implantation.
2.5. Outcome and Assessment
Postoperative assessments were conducted at 1 day, 2 weeks, and 6 months. Monocular and Binocular UCIVA and DCIVA at 80 cm, Binocular UDVA and BCDVA (monocular and binocular), UNVA and DCNVA (monocular and binocular) at 40cm, and Manifest refraction were recorded at 2 weeks and 6 months. IOP and Monocular UDVA were performed at all visits.
2.6. Statistical Analysis
The sample size was determined based on the primary efficacy endpoint: binocular Distance-Corrected Intermediate Visual Acuity (DCIVA) at 66 cm under photopic conditions. Assuming a mean difference of 1.0 line between groups, a standard deviation of 1.2 lines, 85% power, 5% alpha, and a 1:1 allocation ratio, a total of 60 subjects (30 per group) were planned to be enrolled, accounting for a 10% dropout rate, to ensure 52 evaluable subjects (26 per group). Data normality was assessed prior to statistical testing using the Shapiro-Wilk test where applicable. Continuous variables were summarized using descriptive statistics (n, mean, SD, median, minimum, maximum), and categorical variables as frequencies and percentages. Depending on data distribution, parametric (two-sample or paired t-test) or non-parametric tests (Mann-Whitney U or Wilcoxon signed-rank test) were applied for inter- and intra-group comparisons. Results are presented with 95% confidence intervals where applicable, and a p-value <0.05 was considered statistically significant, and analyses were performed using SAS® software version 9.4 or later.
3. RESULTS
The study includes a total of 120 eyes of 60 participants; each group has 30 participants, and all complete the follow-up visits. The demographic details have been mentioned in Table 2.
| Characteristic |
EyecrylTM SERT IOL (N=30) |
TECNIS Eyhance™ IOL (N=30) |
p-value |
|---|---|---|---|
| Age (years), Mean ± SD | 67.3 (8.0) | 65.9(7.4) | 0.4738 |
| Gender, n (%): | - | - | - |
| Eye, n | Right: 60 | Right: 60 | - |
| Left: 60 | Left: 60 | - | |
| Male | 15(50.00) | 18(60.00) | 0.604 |
| Female | 15(50.00) | 12(40.00) | |
| Axial Length (mm) | 23.17 | 23.39 | - |
| Keratometry (D) | −0.54 | −0.69 | - |
| Visual Acuity (logMAR) | - | - | - |
| Monocular UDVA, Mean ± SD | 0.65(0.28) | 0.59(0.31) | 0.278 |
| Monocular BCDVA, Mean ± SD | 0.31(0.26) | 0.26(0.24) | 0.2954 |
| IOP (mmHg), Mean ± SD | 16.12(2.72) | 16.07(2.53) | 0.9171 |
| Sphere (D), Mean ± SD | -0.01(1.97) | -0.74(2.88) | 0.1082 |
| Cylinder (D), Mean ± SD | -0.15(0.82) | -0.15(0.82) | 0.5451 |
| Spherical Equivalent, Mean ± SD | -0.81(3.10) | -0.14(2.21) | 0.1756 |
3.1. Visual Acuity
3.1.1. Distance Corrected Intermediate Visual Acuity (DCIVA)
At 80 cm, monocular DCIVA significantly improved in the EyecrylTM SERT group, from 0.11 ± 0.07 logMAR at 2 weeks to 0.10 ± 0.08 logMAR at 6 months (mean change: -0.01 ± 0.03; p = 0.0156). In the TECNIS Eyhance™ group, monocular DCIVA was 0.15 ± 0.08 logMAR at 2 weeks, which remained stable at 6 months. Binocular DCIVA remained stable in both groups. In the EyecrylTM SERT group, it was 0.06 ± 0.06 logMAR at 2 weeks and 0.07 ± 0.06 at 6 months (mean change: 0.00 ± 0.02; p > 0.05), while in the TECNIS Eyhance™ group, it was unchanged at 0.11 ± 0.09 logMAR. At 6 months, EyecrylTM SERT demonstrated significantly better monocular (p < 0.0001) and binocular (p = 0.0021) DCIVA than TECNIS EyhanceTM (Figs. 1 and 2).
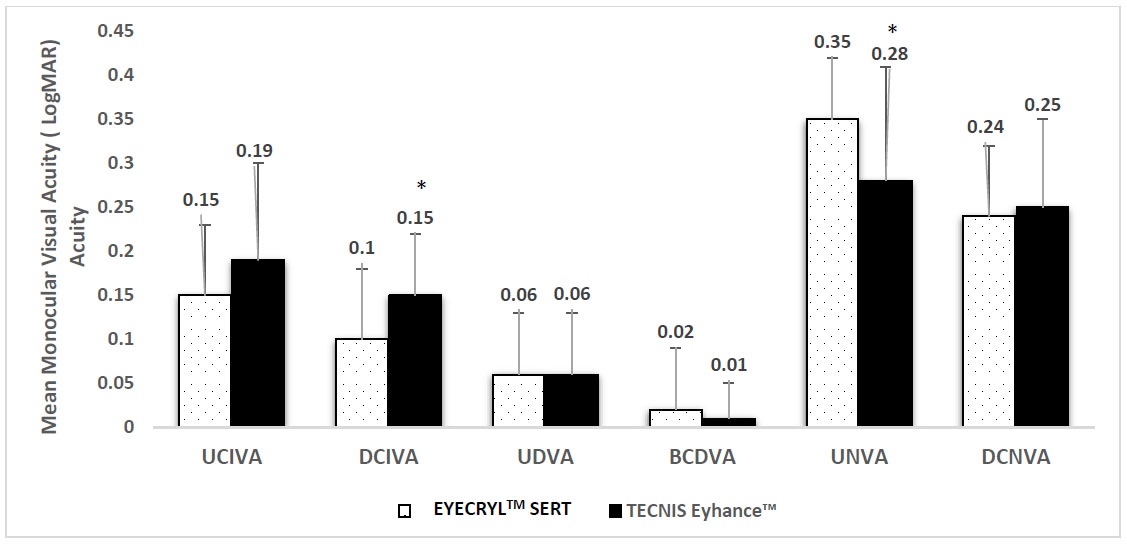
Comparison of monocular visual acuities between EyecrylTM SERT and TECNIS Eyhance™ Intraocular Lenses (IOLs) at 6 months postoperatively. The x-axis represents different types of visual acuity assessed: UCIVA (Uncorrected Intermediate Visual Acuity), DCIVA (Distance-Corrected Intermediate Visual Acuity), UDVA (Uncorrected Distance Visual Acuity), BCDVA (Best-Corrected Distance Visual Acuity), UNVA (Uncorrected Near Visual Acuity), and DCNVA (Distance-Corrected Near Visual Acuity). The y-axis indicates mean visual acuity in logMAR units, where lower values reflect better visual performance. Error bars represent standard deviation. *A p-value of ≤ 0.05 was considered statistically significant.
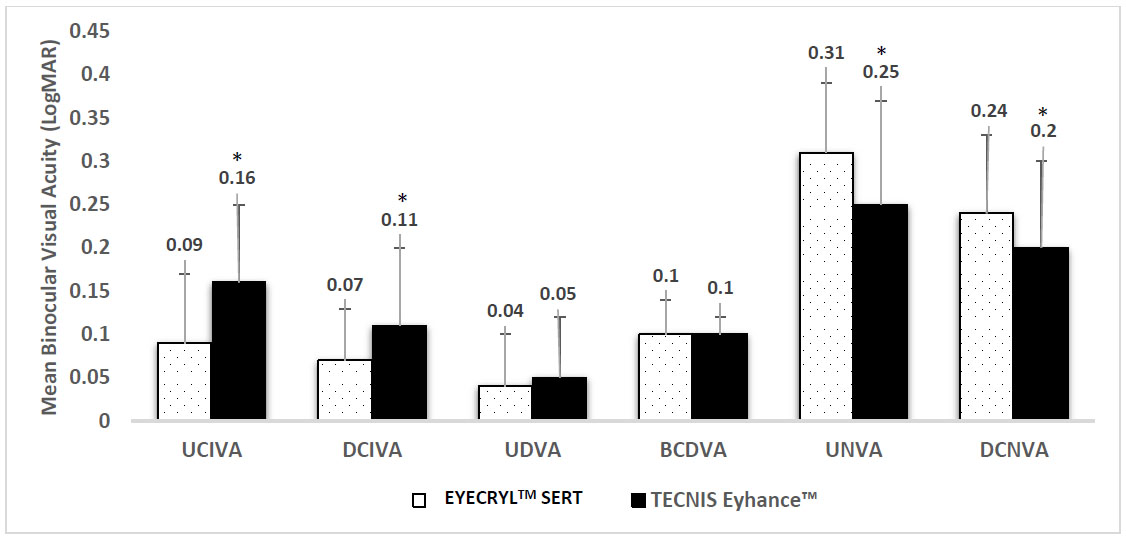
Comparison of binocular visual acuities between EyecrylTM SERT and TECNIS Eyhance™ Intraocular Lenses (IOLs) at 6 months postoperatively. The x-axis represents various types of visual acuity assessed, UCIVA (Uncorrected Intermediate Visual Acuity), DCIVA (Distance-Corrected Intermediate Visual Acuity), UDVA (Uncorrected Distance Visual Acuity), BCDVA (Best-Corrected Distance Visual Acuity), UNVA (Uncorrected Near Visual Acuity), and DCNVA (Distance-Corrected Near Visual Acuity). The y-axis displays mean binocular visual acuity values in logMAR, where lower values indicate better visual performance. Error bars denote standard deviation. *A p-value of ≤ 0.05 was considered statistically significant.
3.1.2. Uncorrected Intermediate Visual Acuity (UCIVA)
Monocular UCIVA at 80 cm showed a slight, non-significant improvement in both groups. In EyecrylTM SERT, mean UCIVA changed from 0.16 ± 0.09 logMAR at 2 weeks to 0.15 ± 0.08 at 6 months (mean change: -0.01 ± 0.04; p = 0.0605). In TECNIS EyhanceTM, it changed from 0.20 ± 0.11 to 0.19 ± 0.11 (mean change: -0.01 ± 0.03; p = 0.125). Binocular UCIVA remained unchanged in both groups. At 6 months, binocular UCIVA was significantly better in the EyecrylTM SERT group (0.09 ± 0.08 vs 0.16 ± 0.09; p = 0.0005), while monocular inter-group difference was not statistically significant (p = 0.0971) (Figs. 1 and 2).
3.1.3. Uncorrected Distance Visual Acuity (UDVA)
Monocular UDVA improved significantly in both groups from baseline to all postoperative time points (p < 0.0001). In EyecrylTM SERT, mean UDVA improved from 0.65 ± 0.28 logMAR preoperatively to 0.19 ± 0.16 on Day 1, 0.09 ± 0.09 at 2 weeks, and 0.06 ± 0.07 at 6 months. TECNIS Eyhance™ showed similar improvement from 0.59 ± 0.31 preoperatively to 0.09 ± 0.11 on Day 1, 0.07 ± 0.10 at 2 weeks, and 0.06 ± 0.07 at 6 months. A statistically significant difference was observed only at Day 1 (p = 0.0237); no significant inter-group differences were found at 2 weeks or 6 months.
Binocular UDVA remained stable in both groups between 2 weeks and 6 months (EyecrylTM SERT: 0.04 ± 0.07 to 0.04 ± 0.06; TECNIS EyhanceTM: 0.03 ± 0.06 to 0.05 ± 0.07; p > 0.05 for both groups), with no significant difference between the groups at 6 months (Figs. 1 and 2).
3.1.4. Best Corrected Distance Visual Acuity (BCDVA)
Monocular BCDVA significantly improved in both groups from baseline. In EyecrylTM SERT, mean BCDVA improved from 0.31 ± 0.26 logMAR preoperatively to 0.03 ± 0.07 at 2 weeks and 0.02 ± 0.07 at 6 months (p < 0.0001). In TECNIS EyhanceTM, values improved from 0.26 ± 0.24 to 0.01 ± 0.04 at 2 weeks and 0.01 ± 0.04 at 6 months (p < 0.0001). Inter-group differences were not statistically significant at either 2 weeks (p = 0.3021) or 6 months (p = 0.4916).
Binocular BCDVA remained stable in both groups over time (EyecrylTM SERT: 0.01 ± 0.04; TECNIS EyhanceTM: 0.01 ± 0.02; p = 1.0000), with no significant inter-group difference at 6 months (p = 0.4841) (Figs. 1 and 2).
3.1.5. Uncorrected Near Visual Acuity (UNVA)
Monocular UNVA remained unchanged in the EyecrylTM SERT group, with a mean of 0.35 ± 0.07 logMAR at both 2 weeks and 6 months. In the TECNIS EyhanceTM group, monocular UNVA improved slightly from 0.29 ± 0.14 to 0.28 ± 0.13 logMAR. At 6 months, inter-group comparison revealed significantly better monocular UNVA in the TECNIS EyhanceTM group (p = 0.0002).
Binocular UNVA remains stable from 2 weeks to 6 months in both IOLs. At 2 weeks, 0.31 ± 0.08 and 0.25 ± 0.12 logMAR for EyecrylTM SERT and TECNIS EyhanceTM, respectively, which remain the same at 6 months (intergroup p=0.004) (Figs. 1 and 2).
3.1.6. Distance-corrected Near Visual Acuity (DCNVA)
Monocular DCNVA is nearly stable from 2 weeks to 6 months in EyecrylTM SERT (0.24 ± 0.8 logMAR; p = 1.00), whereas TECNIS EyhanceTM showed marked improvement from 2 weeks to 6 months (0.26 ± 0.11 to 0.25 ± 0.11; p = 0.03), although no statistical significant change in both groups at 6 months.
Binocular DCNVA remains stable from 2 weeks to 6 months in both IOLs. However, TECNIS EyhanceTM showed better visual acuity in intergroup analysis at 6 months. (0.24 ± 0.9 vs 0.20 ± 0.10 logMAR; p = 0.036) (Figs. 1 and 2).
3.2. Intraocular Pressure
In both groups, Intraocular Pressure (IOP) showed a transient postoperative rise on Day 1, followed by a return to baseline or below. In the EyecrylTM SERT group, IOP increased from 16.12 ± 2.72 mmHg preoperatively to 18.28 ± 6.16 mmHg on Day 1 (p = 0.0247), then decreased to 14.55 ± 3.37 mmHg at 2 weeks (p = 0.0131), and 15.78 ± 2.24 mmHg at 6 months (p = 0.5053).
Similarly, in the TECNIS EyhanceTM group, IOP rose from 16.07 ± 2.53 mmHg to 18.87 ± 4.80 mmHg on Day 1 (p < 0.0001), and returned to 15.28 ± 2.92 mmHg at 2 weeks (p = 0.0726) and 15.90 ± 3.12 mmHg at 6 months (p = 0.7275). Inter-group comparisons at each postoperative time point showed no statistically significant differences (Day 1: p = 0.3900; 2 weeks: p = 0.5875; 6 months: p = 0.9515).
3.3. Refractive Outcomes
Manifest refraction (sphere) remained stable in both groups throughout the follow-up period. In the EyecrylTM SERT group, mean spherical error changed minimally from -0.01 ± 1.97 D preoperatively to 0.06 ± 0.14 D at 2 weeks (p = 0.9530) and 0.03 ± 0.11 D at 6 months (p = 0.8170). In the TECNIS Eyhance™ group, a greater hyperopic shift was observed, from -0.74 ± 2.88 D to -0.04 ± 0.29 D at 2 weeks (p = 0.3219) and -0.03 ± 0.24 D at 6 months (p = 0.2704), though the change was not statistically significant. Inter-group comparisons at both time points showed no significant differences (Fig. 3).
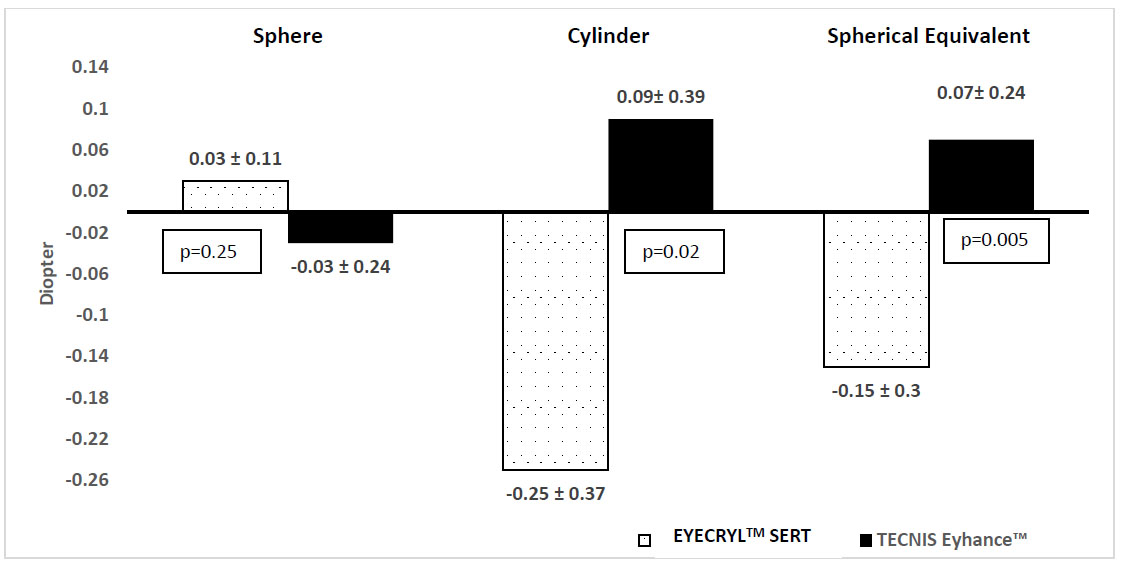
Comparison of mean postoperative refractive outcomes, sphere, cylinder, and Spherical Equivalent (SE), between EyecrylTM SERT and TECNIS Eyhance™ Intraocular Lenses (IOLs) at 6 months. The x-axis represents the refractive parameters, while the y-axis denotes the Diopter (D) values. Bars indicate mean ± standard deviation.
Manifest refraction (cylinder) remained stable in the EyecrylTM SERT group (-0.15 ± 0.82 D to -0.25 ± 0.37 D), with no significant change over time. In contrast, the TECNIS Eyhance™ group demonstrated a statistically significant reduction in refractive cylinder from -0.24 ± 0.91 D preoperatively to -0.10 ± 0.47 D at 2 weeks (p = 0.0060) and to +0.09 ± 0.39 D at 6 months (p = 0.0071). Inter-group comparisons at 2 weeks (p = 0.0357) and 6 months (p = 0.0271) also showed statistically significant differences, indicating better astigmatic correction in the TECNIS Eyhance™ group (Fig. 3).
Manifest refraction (spherical equivalent) improved in both groups; however, the within-group changes were not statistically significant in either group (p>0.05, all visits). In the EyecrylTM SERT group, the spherical equivalent shifted from -0.81 ± 3.10 D preoperatively to -0.16 ± 0.37 D at 2 weeks and -0.15 ± 0.30 D at 6 months. In the TECNIS Eyhance™ group, values changed from -0.14 ± 2.21 D to 0.15 ± 0.26 D at 2 weeks and 0.07 ± 0.24 D at 6 months. Although inter-group comparisons showed statistically significant differences at both postoperative time points (p = 0.0013 and p = 0.0054), the absolute differences in spherical equivalent were small (<0.35 D) and fell within normal postoperative variability. These differences were therefore not clinically meaningful, and both IOLs demonstrated stable and comparable refractive outcomes (Fig. 3).
4. DISCUSSION
The present data is a part of a larger data set derived from a prospective, non-randomized comparative investigation that demonstrated comparable visual performance of EyecrylTM SERT relative to TECNIS Eyhance™ across multiple parameters over a 6-month postoperative period. Both the study arms were demographically similar, with balanced gender distribution and mean ages of 67.3 ± 8.0 years (EyecrylTM SERT) and 65.9 ± 7.4 years (TECNIS EyhanceTM).
The study showcases comparable performance of EyecrylTM SERT and TECNIS Eyhance™ across various visual acuities. At 80 cm, EyecrylTM SERT demonstrated better Distance-Corrected Intermediate Visual Acuity (DCIVA) compared to TECNIS Eyhance™ in both monocular and binocular assessments at 6 months postoperatively, with statistically significant differences (monocular: 0.10 ± 0.08 vs. 0.15 ± 0.07 logMAR; binocular: 0.07 ± 0.06 vs. 0.11 ± 0.09 logMAR; both p < 0.0001). These outcomes surpass those reported for the Isopure IOL (0.23 ± 0.13 logMAR) and the Triumf IOL (0.24 ± 0.10 logMAR) at 4-5 months [9]. The results are also comparable with the LuxSmart EDOF IOL (Bausch + Lomb), which demonstrated monocular DCIVA of 0.08 ± 0.11 logMAR and binocular DCIVA of 0.004 ± 0.11 logMAR at 6 months [10]. In contrast, the Tecnis Symfony IOL achieved slightly better DCIVA at 3 months (monocular: 0.03 ± 0.083 logMAR; binocular: 0.01 ± 0.086 logMAR) [11]. Waring et al. (2024) reported monocular DCIVA values of 0.26 ± 0.08 logMAR (DXR00V) and 0.23 ± 0.06 logMAR (DFR00V), highlighting the favorable performance of both IOLs in the present study [12]. Additionally, 80.65% of subjects implanted with the Isopure 123 IOL achieved binocular DCIVA of 20/25 or better (≤0.1 logMAR) at 80 cm, further underscoring the relevance of intermediate vision optimization in modern IOL designs [13].
Similar to DCIVA, EyecrylTM SERT demonstrated slightly better clinical outcome than TECNIS EyhanceTM for binocular UCIVA at 80cm 6 months postoperatively (0.09 ± 0.08 vs. 0.16 ± 0.09 logMAR; p = 0.0005); however, monocular showed better visual acuity but remained statistically non-significant (0.15 ± 0.08 vs. 0.19 ± 0.11 logMAR; p = 0.0971). These outcomes are in line with those reported for other enhanced or Extended Depth-Of-Focus (EDOF) IOLs. For example, the LuxSmart EDOF IOL (Bausch + Lomb) showed binocular and monocular UCIVA of 0.026 ± 0.12 and 0.11 ± 0.13 logMAR, respectively, at 6 months [10]. Kohnen et al. (2019) reported UCIVA at 80 cm for TECNIS Eyhance™ as 0.01 ± 0.077 logMAR (binocular) and 0.04 ± 0.087 logMAR (monocular) at 3 months, comparable to the current findings [11]. Additionally, Ganesh et al. (2021) reported a 6-month binocular UCIVA of 0.04 ± 0.08 logMAR with the AT LARA 829MP EDOF IOL [14].
In the present study, both IOL groups demonstrated significant improvements in monocular and binocular UDVA from baseline to 6 months postoperatively. In the EyecrylTM SERT group, mean monocular UDVA improved from 0.65 ± 0.28 logMAR preoperatively to 0.06 ± 0.07 at 6 months. Similarly, the TECNIS Eyhance™ group showed an improvement from 0.59 ± 0.31 to 0.06 ± 0.07 logMAR. Binocular UDVA also remained stable from 2 weeks to 6 months in both groups (EyecrylTM SERT: 0.04 ± 0.07 to 0.04 ± 0.06; TECNIS EyhanceTM: 0.03 ± 0.06 to 0.05 ± 0.07). These findings are in line with prior literature. Waring et al. (2024) reported mean monocular UDVA at 6 months of -0.05 ± 0.10 logMAR for DXR00V eyes and 0.04 ± 0.13 logMAR for DFR00V eyes, which is comparable to the 0.06 ± 0.07 logMAR observed in both EyecrylTM SERT and TECNIS Eyhance™ arms of the present study [12]. Similarly, in a study comparing femtosecond laser-assisted with conventional phacoemulsification using TECNIS Symfony IOL, documented mean UDVA values of 0.11 ± 0.12 LogMAR (Phaco group) and 0.09 ± 0.12 logMAR (Femto group) at 3 months postoperatively (p = 0.164), suggesting a similar performance compared to the current findings, where 2-week UDVA values were 0.09 ± 0.09 logMAR in SERT and 0.07 ± 0.10 logMAR in TECNIS group [15]. However, Paik et al. (2020) reported better outcomes with the Tenis Symfony IOL, achieving a mean UDVA of -0.10 ± 0.07 logMAR at 3 months postoperatively [16]. Overall, the UDVA outcomes in the present study are consistent with or better than several published results for comparable extended depth-of-focus and enhanced monofocal IOLs.
The BCDVA value for IOL groups shows demonstrated significant improvement from 2 weeks to monocular (0.02 ± 0.07 logMAR vs 0.01 ± 0.04 logMAR; p=0.491) and binocular BCDVA at postoperatively, with no statistically significant differences between them at 6 months postoperatively. At 6 months, the mean improvement was -0.29 ± 0.27 LogMAR in the EyecrylTM SERT group and -0.25 ± 0.23 LogMAR in the TECNIS Eyhance™ group (both p < 0.0001), reflecting excellent recovery of corrected distance vision in both arms. Binocular BCDVA remained stable at 2 weeks and 6 months postoperatively in both groups, with mean values of approximately 0.01 ± 0.2-0.4 LogMAR, consistent with findings reported by Xu et al. (2022) [15].
In contrast, TECNIS Eyhance™ outperformed EyecrylTM SERT in uncorrected near visual acuity. At 6 months, for both monocular and binocular UNVA TECNIS Eyhance™ showed better outcomes than EyecrylTM SERT (0.35 ± 0.07 vs 0.28 ±0.13; p=0.0002 and 0.31 ± 0.08 vs 0.25 ±0.12; p=0.0046, respectively). For monocular distance corrected near visual acuity at 6 months, both IOLs performed equally (0.24 ± 0.08 vs 0.25 ±0.10; p=0.387). However, for binocular DCNVA TECNIS Eyhance™ performed slightly better than EyecrylTM SERT (0.24 ± 0.09 vs 0.20 ±0.10; p=0.036). Comparable data from the literature further contextualize these findings. At 6 months, LuxSmart EDOF IOL yielded monocular and binocular UNVA of 0.31 ± 0.15 and 0.22 ± 0.13 logMAR, respectively, while DCNVA was 0.37 ± 0.16 (monocular) and 0.28 ± 0.12 logMAR (binocular) [10]. Similarly, Tecnis Symfony demonstrated monocular and binocular UNVA of 0.30 ± 0.145 and 0.22 ± 0.153 logMAR, with corresponding DCNVA values of 0.30 ± 0.144 and 0.23 ± 0.126 logMAR. These published outcomes suggest that both LuxSmart and Tecnis Symfony offer comparable near visual performance to TECNIS EyhanceTM, and marginally better outcomes than EyecrylTM SERT.
Postoperative Intraocular Pressure (IOP) remained within physiological limits in both groups throughout the study period, with no significant inter-group differences observed at any visit (p > 0.001 for all), consistent with previous reports [17-19]. Spherical equivalent values favored EyecrylTM SERT at both 2 weeks and 6 months, with mean values of -0.16 ± 0.37 D and -0.15 ± 0.30 D, respectively, compared to -0.15 ± 0.26 D and -0.07 ± 0.24 D in TECNIS Eyhance™ (p = 0.0013 and p = 0.0054, respectively). These outcomes are in line with previously reported results for enhanced monofocal and EDOF IOLs, including TECNIS Eyhance™ (-0.02 ± 0.40 D) [20], TECNIS Symfony OptiBlue (-0.21 ± 0.30 D), and TECNIS Synergy (0.00 ± 0.50 D) [12].
This study has several limitations. Its non-randomized, single-center design may introduce selection bias and limit generalizability. The six-month follow-up restricts assessment of long-term outcomes such as refractive stability and sustained visual benefits. As both eyes from the same patient were included in monocular analyses, potential inter-eye correlation may exist. However, the primary efficacy endpoint of the parent study was binocular and analyzed at the subject level. Additionally, the small sample size may lack power to detect subtle effects or rare complications. Larger, randomized, multicenter studies with extended follow-up are needed to confirm and build on these findings.
CONCLUSION
Both intraocular lenses provided significant improvements in visual acuity and refractive outcomes following cataract surgery. EyecrylTM SERT was more effective in enhancing intermediate visual acuity and maintaining refractive stability, while TECNIS Eyhance™ offered better performance near vision. Distance vision outcomes were comparable between the two groups, with no significant differences in safety parameters over 6 month of study period.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: All authors contributed to the study conception and design. B.J.: Data collection was performed; S.G., M.K., R.P., and B.J.: Formal analysis was performed; S.G.: Resources and supervision were provided; B.J.: The manuscript draft was prepared, and all authors read and approved the final manuscript.
All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| BCDVA | = Best-Corrected Distance Visual Acuity |
| DCIVA | = Distance-Corrected Intermediate Visual Acuity |
| DCNVA | = Distance-Corrected Near Visual Acuity |
| EDOF | = Extended Depth of Focus |
| ETDRS | = Early Treatment Diabetic Retinopathy Study |
| IOL | = Intraocular Lens |
| IOP | = Intraocular Pressure |
| PCO | = Posterior Capsular Opacification |
| UCIVA | = Uncorrected Intermediate Visual Acuity |
| UDVA | = Uncorrected Distance Visual Acuity |
| UNVA | = Uncorrected Near Visual Acuity |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from Nethradhama Super Specialty Eye Hospital, Institutional Ethical Committee (IEC/IRB No. 2022/12).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants after providing a detailed explanation of the study protocol.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGEMENTS
The authors acknowledge Dr KDS and Dr VUK for their valuable contribution to the study.

