All published articles of this journal are available on ScienceDirect.

Emergent Ophthalmic Disease Knowledge among Non-Ophthalmologist Healthcare Professionals in the Western Region of Saudi Arabia: Cross-Sectional Study
Authors Info & Affiliations
Abstract
Background:
Patients with emergent ophthalmic diseases are likely to be examined by healthcare providers before an ophthalmologist, so it is essential that nonspecialists have adequate knowledge for recognition and preliminary diagnosis.
Objectives:
To assess knowledge of retinal detachment, acute angle-closure glaucoma, temporal arteritis, and central retinal artery occlusion among non-ophthalmologist healthcare professionals.
Methods:
We conducted an observational cross-sectional study of 351 healthcare workers, including medical residents, nurses, pharmacists, and optometrists, in western Saudi Arabia using a self-report questionnaire.
Results:
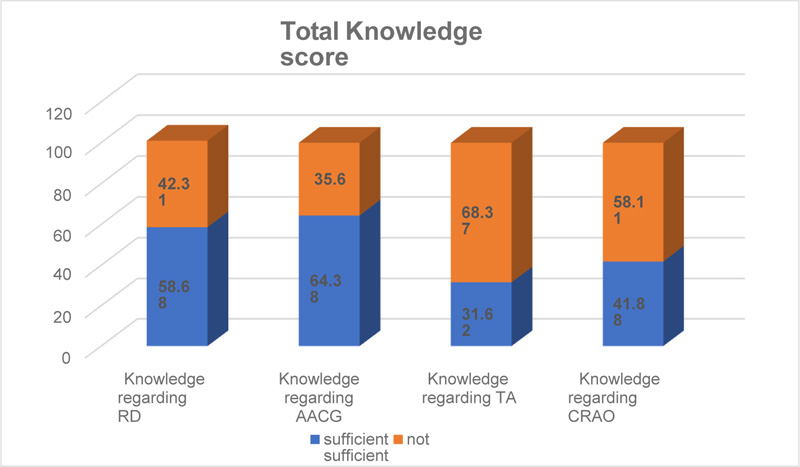
Total knowledge scores were 75.21% for retinal detachment and 74.9% for acute angle-closure glaucoma, but only 44.15% for temporal arteritis and 41.88% for central retinal artery occlusion. Stepwise logistic regression revealed that level of education was the most significant factor influencing knowledge of different eye diseases.
Conclusion:
Ophthalmologists are encouraged to promote greater awareness and provide other healthcare professionals with the knowledge required to recognize emergent eye diseases for early detection.
1. INTRODUCTION
Visual Impairment (VI) is a major global health and social burden. According to 2020 estimates, 43.3 million individuals worldwide are legally or clinically blind, and another 295 million have moderate to severe visual impairment, mostly adults older than 50 years [1]. Furthermore, this number is predicted to reach 360 million by 2050 [1]. In Saudi Arabia, the overall rate of VI is 10–20 times that of the United States [2]. According to evidence-based studies, the most common cause of VI and blindness in Saudi Arabia is cataracts, followed by diabetic retinopathy [2]. Maake et al. [3] reported that error of refraction, cataract, and glaucoma are the main causes of VI, so error correction and cataract surgery can greatly reduce the burden of visual loss. Moreover, 12.6% of total blindness cases worldwide are in Eastern Mediterranean countries, including Saudi Arabia [4], so there is a great need for more effective prevention and screening in this region.
Few patients with early-stage VI will first seek treatment from an ophthalmologist. Thus, most patients will first visit a nonspecialist, possibly for another ailment. Therefore, greater awareness and knowledge regarding emergent eye diseases such as cataracts, diabetic retinopathy, glaucoma, and central retinal artery occlusion among nonspecialists could facilitate early diagnosis and treatment, potentially reducing the emotional, social, and economic burdens of blindness and VI [5-7]. Promoting the importance of regular eye care and providing sufficient knowledge to nonspecialists about emergent eye disorders is thus a critical responsibility of ophthalmologists.
Factors such as age, educational level, socioeconomic status, and sex may influence the level of awareness and knowledge regarding emergent eye diseases [8]. For instance, the elderly may believe that decreased vision and blindness are normal during aging [9]. Alternatively, Bandar [10] reported that study participants with high socioeconomic status were more aware of eye disease and had positive attitudes toward eye care. Mohammad et al. [11] found that eye care education is the main determinant of knowledge among patients and that this was mostly imparted by primary physicians, underscoring the importance of physician training for detection and early screening of emergency eye diseases. The prevalence of VI is associated with the rates of non-communicable diseases such as hypertension, diabetes, and cardiovascular diseases, smoking, a sedentary lifestyle, and poor dietary habits [10, 12].
Several studies have assessed the knowledge and awareness of eye diseases such as cataracts, refractive errors, and diabetic retinopathy among Saudi Arabian patients and primary healthcare professionals. However, no studies have addressed the knowledge of emergent and other eye diseases such as retinal detachment (RD), acute angle-closure glaucoma (AACG), giant cell temporal arteritis (TA), and central retinal artery occlusion (CRAO) among non-ophthalmologists healthcare professionals. This study aims to assess such awareness and knowledge among a cross-section of non-ophthalmologist healthcare professionals in Saudi Arabia using a self-administered online questionnaire specifically designed for this task [6].
2. MATERIALS AND METHODS
2.1. Participants
This observational cross-sectional study was conducted in western Saudi Arabia from March to July 2021. A self-administrated questionnaire was designed in English as the majority of healthcare workers in Saudi Arabia are English speaking. Consent was obtained from all participants before distributing the questionnaire, and the participants were ensured of confidentiality and the voluntary nature of study inclusion. Ethical approval was obtained from the ethics committee of the General Directorate of Health Affairs in Madinah, and the study was conducted in accordance with the deceleration of Helsinki. A sample size of 351 was determined as adequate for the study, and the study cohort was selected by convenience sampling. Application for inclusion was closed after recruitment of 351 participants after exclusion of incompleted questionnaires (n=49). The sample of healthcare professionals included physicians, nurses, dentists, pharmacists, and optometrists of both sexes who agreed to complete the questionnaire after providing informed written consent.
2.2. Questionnaire
A self-administered questionnaire was designed by Uhr et al. [6] for evaluating awareness and knowledge regarding emergent eye diseases among healthcare professionals. The applicability of this questionnaire was assessed in a pilot study which included 10% of the sample size. These data were not included in the final analysis. The questionnaire was composed of three parts: a section recording participant sociodemographic characteristics (age, sex, level of education, place of work, healthcare, occupation, history of eye disease, and time since the last eye exam), a section including questions regarding awareness, and a section on the knowledge of RD, AACG, TA, and CRAO. Items on awareness were answered as Aware or Unaware, items on symptoms and treatment as Yes, No, or I don’t know, and items on pathophysiology and complications by five explicit options. A knowledge score for each disease was calculated, adding two points for each correct answer and one for each “I don’t know” response, while incorrect answers received no points. Participants with a score of 8 or more for a particular subject (75% or more) were considered to have sufficient awareness and knowledge, while those with an average score of less than 8 were considered to have insufficient awareness and knowledge except for glaucoma, where a score of 6 or more (75% or more) was considered sufficient. Mean scores were calculated for each disorder to gauge general awareness and knowledge.
2.3. Statistical Analyses
The sample size was estimated using the Epidemiological Information Package (EPI INFO) version 3.5.3 (21), assuming a frequency of 20% with a confidence interval of 95% and statistical power of 80%. Data were analyzed using Statistical Package for Social Science version 28 2021 (SPSS Inc., Chicago, IL). Quantitative data are presented as mean ± standard deviation (SD) and qualitative data as count and proportions (%). Means were compared by analysis of variance. A P < 0.05 (two-tailed) was considered significant.
3. RESULTS
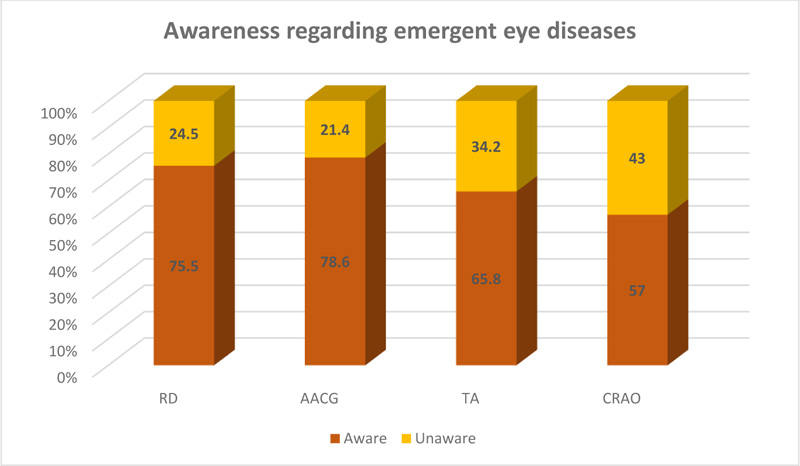
Among the 351 respondents to the questionnaire, of which well over half were clinicians or nurses, almost half reported never having an eye exam, and only 79 (22.5%) reported having an eye examination in the past two years, suggesting insufficient concern for personal eye care even among nonspecialist healthcare professionals. However, the total incidence of emergent eye diseases among the participants was also low (6%), with the most frequent being glaucoma and cataract (Table 1). Awareness of RD and AACG were also deemed sufficient (>75%), but awareness concerning TA and CRAO was insufficient (65.8% and 57%, respectively) (Fig. 1).
About 75% of participants demonstrated sufficient knowledge on the pathophysiology, symptoms, methods of management, and complications of RD (Table 2) and AACG (Table 3). However, well below 50% of participants demonstrated sufficient knowledge levels on TA (Table 4) and CRAO (Table 5). In the RD section, 68.4% of participants correctly defined the disease as “When the cells that detect light in the back of your eye become separated from the layer underneath them,” and most participants were also aware of symptoms (69.5%), the need for urgent assessment (74.6%), and that RD could cause loss of vision (79.2%) (Fig. 2). However, large minorities mistakenly believed that pills or eye drops were treatments and that all patients required urgent intervention. Nonetheless, the overall mean score (8.8034 ± 2.09) was considered sufficient, and there was no significant difference between awareness level and knowledge score (P = 0.930). Overall, 69.5% of participants correctly answered that pain and blurred vision are common symptoms of AACG, and 70.7% knew that AACG might cause vision loss (Table 3).
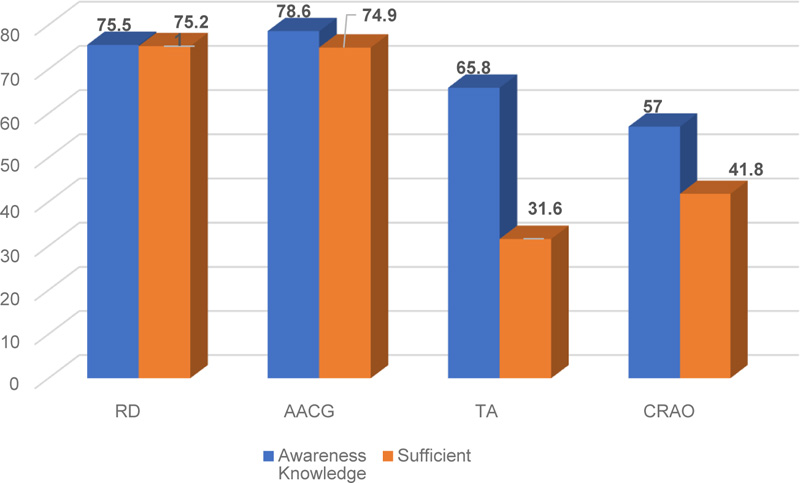
In contrast, less than half of the participants correctly identified the underlying pathophysiology of TA, and the overall level of knowledge regarding definition, symptoms, management, and complications was only 44.15% (Table 5). Furthermore, only 49% correctly identified jaw pain, 51.4% scalp pain, 32.8% pain while brushing your hair, and 20.6% fever and weight loss as symptoms. Similarly, the total mean knowledge score for CRAO was low (6.712 ± 2.33) (Table 6). There were also significant differences between awareness level and knowledge scores for both disorders (P < 0.0001 and P < 0.0006, respectively), indicating that guessing could not account for awareness and knowledge (Fig. 3).
The level of awareness regarding retinal detachment was significantly associated with respondent age >50 (P = 0.042), educational level (Master’s and above) (P < 0.0001), and consultant position (P < 0.0001). Moreover, consultants and those with a Master’s degree were more aware of different eye diseases than the remainder of the participants (both P < 0.0001) (Table 6). Males were significantly more aware of temporal arteritis than females (P = 0.036), as were participants <30 years (P = 0.034). Stepwise logistic regression identified the level of education as the strongest factor influencing the level of knowledge on these eye diseases (Table 7).
| Characteristic | Value | |
|---|---|---|
|
Age (years) Mean± SD (minimum-maximum) |
30.5128±5.788 (19–62) |
|
| Items | Number | % |
|
Age group (years) <30 30–49 ≥50 Total |
200 143 8 351 |
56.9 40.7 2.2 100 |
|
Sex Male Female Total |
175 176 351 |
49.9 50.1 100 |
|
Level of education: Diploma Bacheloria Board Board certified Masters PhD Other Total |
24 154 99 58 11 4 1 351 |
6.8 43.9 28.2 16.5 3.1 1.1 0.3 100 |
|
Profession Resident Nurse Consultant Specialist Pharmacist Optometrist Total |
135 112 29 29 26 20 351 |
38.5 31.9 8.3 8.3 7.4 5.7 100 |
|
Place of work Ophthalmology Emergency General surgery Family medicine Primary healthcare Internal medicine Other (pharmaceutical) Total |
29 157 13 79 32 31 6 347 (4 missed) |
8.4 45.2 3.7 22.8 9.2 8.9 1.7 100 |
|
Have you been diagnosed with any of the following eye diseases? • Glaucoma • Cataract • Diabetic retinopathy • Central retinal artery occlusion • Retinal tear/detachment • No Other (Keratoconus/Myopia/Squint) |
21 11 13 3 10 307 6 |
6 3.1 3.7 0.9 2.8 87.5 1.7 |
|
The last time you had an eye exam • Never • Within the past two years • Between 2–5 years ago • Greater than 5 years ago • I don’t know Total |
175 79 35 20 42 351 |
49.9 22.5 10 5.7 12 100 |
| Item | Number of Responses (n = 351) | % |
|---|---|---|
|
Retinal detachment is • When the cells that detect light in the back of your eye become separated from the layer underneath them • When the lens in your eye is ripped away from its normal place • When the optic nerve that connects your eye to your brain is torn in half • I don’t know Total |
240 35 5 71 351 |
68.4 10 1.4 20.2 100 |
|
Seeing bright flashing lights can be a symptom of retinal detachment. • Yes • No • I don’t know Total |
244 12 95 351 |
69.5 3.4 27.1 100 |
|
Retinal detachment can be cured if you take medication (pills or eye drops) immediately after it happens. • Yes • No • I don’t know Total |
50 160 141 351 |
14.2 45.6 40.2 100 |
|
All patients with acute retinal detachment must have an urgent assessment (laser surgery). • Yes • No • I don’t know Total |
262 21 68 351 |
74.6 6 19.4 100 |
|
All patients with chronic retinal detachment must have an urgent intervention. • Yes • No • I don’t know Total |
162 93 96 351 |
46.2 26.5 27.4 100 |
|
Can the disease cause vision loss? • Yes • No • I don’t know Total |
278 8 65 351 |
79.2 2.3 18.5 100 |
|
Knowledge score Mean ± SD (minimum-maximum) |
8.8034±2.09 (2–12) |
|
|
Pass rate • Sufficient • Not • Relation with just knowing. (P-value) |
264 (75.21%) 87 (24.79%) 0.930 |
|
Table 3.
| Item | Number of Responses (n = 351) | % |
|---|---|---|
|
Acute angle-closure glaucoma is • When something gets caught in your eye, and you cannot open your eye • When the pressure inside your eye rapidly becomes very high • When an infection inside your eye causes your eye to rapidly become swollen • I don’t know Total |
240 35 5 71 351 |
68.4 10 1.4 20.2 100 |
|
Pain and blurry vision are common symptoms in acute angle-closure glaucoma. • Yes • No • I don’t know Total |
244 12 95 351 |
69.5 3.4 27.1 100 |
|
Acute angle-closure glaucoma only needs glaucoma lowering drops as a treatment. • Yes • No • I don’t know Total |
50 160 141 351 |
14.2 45.6 40.2 100 |
|
Can the disease cause vision loss? • Yes • No • I don’t know Total |
248 18 85 351 |
70.7 5.1 24.2 100 |
|
Knowledge score Mean ± SD (minimum-maximum) |
6.23±1.84 (2-8) |
|
|
Pass rate • Sufficient • Not • Relation with just knowing. (P-value) |
263(74.9%) 88 (24.1%) 0.245 |
|
| Item | No (n = 351) | % |
|---|---|---|
|
Temporal arteritis is • A disease that causes blindness in both eyes slowly over several years by cutting off blood to the eyes • A disease in elderly individuals that can cause blindness in both eyes several days apart if not treated properly • A condition that causes blindness in both eyes in children most commonly after injury to the side of the head • I don’t know Total |
62 158 8 123 351 |
17.7 45 2.3 35 100 |
|
Temporal arteritis is common in young patients. • Yes • No • I don’t know Total: |
70 128 153 351 |
19.9 36.5 43.6 100 |
|
Patients with temporal arteritis may complain of • Pain in your jaw • Scalp pain • Pain while brushing your hair • Flashing lights/curtains • Fever, night sweats, weight loss • Light sensitivity (can’t tolerate light) • Floaters • I don’t know |
172 180 115 78 72 89 29 72 |
49 51.4 32.8 22.3 20.6 25.4 8.3 20.6 |
|
All patients with temporal arteritis must have an emergent assessment. • Yes • No • I don’t know Total: |
235 20 95 350 |
67 5.7 27.1 99.7 |
|
Can the disease cause vision loss? • Yes • No • I don’t know Total: |
227 16 108 351 |
64.7 4.6 30.8 100 |
|
Knowledge score Mean ± SD (minimum-maximum) |
7.025±2.513 (2-12) |
|
|
Pass rate • Sufficient • Not • Relation with just knowing. (P-value) |
155 (44.2%) 196 (55.8%) <0.0001* |
|
Table 5.
| Item | Number of Responses (n = 351) | % |
|---|---|---|
|
CRAO is • When blood is prevented from leaving your eye and builds up inside of the eye • A sudden increase in pressure inside your eye • A sudden loss of vision from decreased blood going into the eye • I don’t know Total |
57 10 152 132 351 |
16.2 2.8 43.3 37.6 100 |
|
People with CRAO often have painful red-eye. • Yes • No • I don’t know Total: |
149 56 146 351 |
42.5 16 41.6 100 |
|
Check all risk factors you know about CRAO. • Diabetes mellitus • Hypertension • High lipids • Cataract • Glaucoma |
110 230 117 45 275 |
31.3 65.5 33.3 12.8 78.3 |
|
All patients with CRAO must have an emergent assessment. • Yes • No • I don’t know Total: |
200 15 136 351 |
56.9 4.3 38.74 100 |
|
Can the disease cause vision loss? Yes • No • I don’t know Total: |
203 16 132 351 |
57.8 4.6 37.6 100 |
|
Knowledge score Mean ± SD (minimum-maximum) |
6.712±2.33 (2-11) |
|
|
Pass rate • Sufficient • Not • Relation with just knowing. (P-value) |
147 (41.8%) 204 (58.1%) <0.0006* |
|
| Factor | RD knowledge | AACG knowledge | TA knowledge | CRAO knowledge |
|---|---|---|---|---|
| Age | ||||
| • <30 | 8.57 ± 2.07 | 5.875 ± 1.77 | 7.326 ± 2.52 | 6.630 ± 2.25 |
| • 30–49 | 9.06 ± 2.12 | 6.035 ± 1.96 | 6.612 ± 2.48 | 6.755 ± 2.45 |
| • >50 | 9.75 ± 1.38 | 6.50 ± 1.511 | 6.875 ± 1.80 | 8.00 ± 2.13 |
| P-value | 0.042* | 0.513 | 0.034* | 0.257 |
| Gender | ||||
| • Male | 9.034 ± 2.02 | 5.39 ± 1.57 | 6.57 ± 2.10 | 6.148 ± 2.02 |
| • Female | 8.573 ± 2.14 | 4.948 ± 1.58 | 6.15 ± 2.29 | 6.136 ± 1.99 |
| P-value: | 0.063 | 0.233 | 0.036* | 0.248 |
| Occupation | ||||
| • Resident | 9.511 ± 1.610 | 5.518 ± 1.348 | 7.311 ± 2.08 | 6.903 ± 1.864 |
| • Nurse | 7.535 ± 1.912 | 4.392 ± 1.561 | 5.162 ± 1.89 | 5.169 ± 1.576 |
| • Consultant | 10.655 ± 1.142 | 6.482 ± 1.021 | 7.275 ± 1.849 | 7.448 ± 1.824 |
| • Specialist | 9.482 ± 2.046 | 5.392 ± 1.448 | 6.034 ± 2.47 | 6.482 ± 2.063 |
| • Pharmacist | 7.384 ± 2.299 | 4.230 ± 1.903 | 5.730 ± 1.45 | 4.538 ± 1.654 |
| • Optometrist | 9.300 ± 2.05 | 6.15 ± 0.988 | 6.600 ± 2.11 | 6.150 ± 2.13 |
| P-value: | <0.001 | <0.001 | <0.001 | <0.001 |
| Educational level | ||||
| • Diploma | 7.833 ± 2.352 | 4.00 ± 1.744 | 6.375 ± 1.883 | 5.750 ± 2.06 |
| • Bacheloria | 8.136 ± 2.048 | 4.857 ± 1.514 | 5.836 ± 1.985 | 5.571 ± 1.983 |
| • Board | 9.212 ± 1.757 | 5.424 ± 1.464 | 7.131 ± 2.301 | 6.575 ± 1.807 |
| • Board certified | 9.931 ± 2.042 | 5.824 ± 1.513 | 6.172 ± 2.241 | 6.827 ± 2.078 |
| • Masters | 10.181 ± 1.078 | 6.727 ± 0.646 | 7.818 ± 2.358 | 7.272 ± 1.420 |
| • PhD | 10.00 ± 1.632 | 5.00 ± 1.632 | 7.250 ± 1.707 | 6.250 ± 1.707 |
| P-value: | <0.001 | <0.001 | <0.001 | <0.001 |
| Sociodemographic characteristic | Adjusted OR (95% Confidence interval) | |||
|---|---|---|---|---|
| RD knowledge | AACG knowledge | TA knowledge | CRAO knowledge | |
| Age | 1.646 0.974–2.781 |
0.895 0.566–1.415 |
0.561 0.351–0.895 |
0.769 0.482–1.227 |
| Gender | 0.769 0.462-1.279 |
0.742 0.469–1.173 |
0.782 0.498–1.228 |
1.290 0.818–2.035 |
| Level of education |
1.881 1.391–2.542* |
1.739 1.340–2.258* |
1.619 1.265–2.072* |
1.976 1.528–2.55* |
| Profession | 0.848 0.716–1.005 |
1.017 0.861–1.200 |
0.767 0.650–0.906 |
0.819 0.691–0.971 |
4. DISCUSSION
The government of Saudi Arabia has allocated a relatively large budget for ophthalmic care due to the high rates of blindness and visual impairment compared to many western counties, and this funding is expected to have a positive impact on VI prevalence in the coming years [2]. However, early diagnosis and treatment are still essential, and patients are more likely to visit doctors, pharmacists, and optometrists before an ophthalmologist, so these healthcare professionals must have adequate awareness and knowledge to recognize these disorders and refer patients to specialists.
To our knowledge, this is the first study to assess the awareness and knowledge of emergent eye diseases among non-ophthalmologist healthcare professionals in Saudi Arabia. The main finding is that overall awareness and knowledge scores vary markedly among different eye diseases. For instance, awareness and knowledge levels for retinal detachment and acute angle-closure glaucoma were substantially higher than for temporal arteritis and central retinal artery occlusion. However, there were still misconceptions regarding the symptoms and treatments for RA and AACG, underscoring the importance of better training to recognize and treat these diseases. For instance, blindness may result if the family physician or resident does not refer a patient with RD or early-stage diabetic retinopathy to an ophthalmologist. Furthermore, sufficient training of nonspecialists maybe even more critical during the current Covid-19 pandemic as many physicians are working in unfamiliar health units [13].
Knowledge and awareness levels differ substantially within and across the study according to age, nationality, and sex, among other factors. In the current study, awareness of different emergent eye diseases also differed by age group, with respondents 50 years older more aware of retinal detachment than other age groups and those younger than 30 years significantly more aware of temporal arteritis. Bandar [10] found that individuals in the general Saudi population between 30 and 50 years of age were more aware of different eye diseases than other age groups, while Islam et al. [12] found that older respondents from Bangladesh were less aware of eye diseases than younger respondents; however, overall awareness regarding different eye diseases was poor and was more marked among respondents of low socioeconomic status. In the current study, there was no significant difference in knowledge scores between males and females, while a study from Tanzania reported a significant difference between male and female healthcare workers [14].
Knowledge levels on RD pathophysiology, symptoms, management, and complications were generally acceptable, likely because RD is one of the more common eye diseases diagnosed in the emergency department, especially in patients 50 years and older [15] due to the more frequent history of cataract surgery and higher prevalence of myopia [16]. Thus, nurses and physicians are likely to encounter RD during training or work history. General knowledge on AACG was also acceptable, although slightly lower than in a recent cross-sectional survey among healthcare workers in Nigeria. However, it was found that their knowledge was theoretical and that they did not have any practical experience with these diseases [17]. Similarly, in a study from Togo, almost all respondent healthcare professionals knew the definition of glaucoma, but only 51.5% demonstrated good general knowledge of the disease [18]. Thus, knowledge levels vary markedly across countries. Indeed, Khawaji et al. [19] found that 91% of professional respondents demonstrated good knowledge of glaucoma, while Onabolu and Bodunde [20] found that only 42.5% of primary healthcare had a good working knowledge of glaucoma.
Proper treatment is essential for preventing glaucoma-related blindness, so it is important to raise awareness and knowledge levels among both the general population and healthcare professionals regarding risk factors and encourage regular assessments [21]. However, glaucoma is still not screened extensively, which may explain the lack of experience among professionals in certain countries, especially those lacking basic ophthalmology equipment in primary health units and the expertise required for diagnosis and management [14]. Sukati et al. [22] also reported a lack of professional knowledge on standard optometric referral guidelines in Swaziland.
A relatively high fraction of participants (44.15%) were aware of temporal arteritis, while Uhr et al. [6] found that only 5.1% of non-healthcare workers were familiar with the disease. However, the overall knowledge score was still insufficient among healthcare workers in the current study. Only 64.7% of respondents correctly answered that TA could cause vision loss, which is considered one of the most important ophthalmology emergencies requiring early and aggressive management [23]. Furthermore, few participants were familiar with the common symptoms (pain in your jaw, scalp pain, pain while pushing your hair, fever, night sweats, and weight loss) and frequently responded with ”I don’t know.”
The following American College of Rheumatology 1990 criteria are considered the gold standard for the diagnosis of giant cell arteritis (GCA) [24]: age above fifty years old, sudden onset of headache, tenderness over the temporal artery, elevation in erythrocyte sedimentation rate, and temporal artery biopsy positive for GCA [24]. As a result, a rheumatologist may be more equipped than other specialists to diagnose the disease in an emergency.
Stepwise logistic regression analysis revealed the level of education as the strongest factor influencing the level of knowledge on different ophthalmic diseases, consistent with Amedomeet al.’s study, which found a significant correlation between knowledge and level of education [18].
CONCLUSION
These findings suggest that nonspecialist healthcare professionals require more information from ophthalmologists on the diagnostic criteria and management of emergent eye diseases to reduce the burden of VI and blindness.
LIST OF ABBREVIATIONS
| AACG | = Acute Angle Closure Glaucoma |
| BPDES | = Bangladesh Population-Based Diabetes and eye Study |
| CRAO | = Central Retinal Artery Occlusion |
| SD | = Standard Deviation |
| TA | = Temporal Arteritis |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics approval was taken from the Research Ethics Committee in General Directorate of Health Affairs in Madinah, Madinah, with approval number 21-2021.
HUMAN AND ANIMAL RIGHTS
No Animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All research participants signed a written informed consent form.
STANDARDS OF REPORTING
STROBE guidelines were followed for this observational cross-sectional study.
AVAILABILITY OF DATA AND MATERIALS
Not available.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

