All published articles of this journal are available on ScienceDirect.

Analysis of the Ophthalmological Manifestations of Diagnosed Cases of Idiopathic Intracranial Hypertension
Abstract
Purpose:
The purpose of this study was to explore the ophthalmological involvement in diagnosed cases of Idiopathic Intracranial Hypertension (IIH).
Methods:
Case series of all patients diagnosed with IIH from October 2012-2014 at the Neurology Department of Amrita Institute of Medical Sciences were prospectively analysed. Analysis was done for 35 patients who fulfilled the updated diagnostic criteria.
Results:
80% of the patients were women with a mean age of 34.5. The chief complaint was a throbbing headache in 85.7%.The least common complaints were tinnitus, phonophobia, and photophobia, and one patient had right facial paresis. All patients had well-preserved visual acuity. 30 patients had normal extraocular movements, bilateral abduction restriction was found in 4 patients, and one was reported to be with third and sixth nerve paresis. 22 patients were in Obese class I. CSF opening pressure was elevated in all patients. 80% had Grade 1 papilledema. Enlargement of blindspot and peripheral constriction of fields were commonly seen. 41.4% of patients showed inferior RNFL thickness to be the most affected. A statistically significant association was found between the grade of papilloedema and the visual field.
Conclusion:
All our patients had papilledema clinically, with well-preserved central vision. Visual field defects were found, which showed a positive correlation with the severity of papilledema, showing the visual field to be a sensitive indicator. Contrary to expectation, an increase in RNFL on OCT was not a universal finding in our patients despite clinically observable papilledema.
1. INTRODUCTION
Idiopathic intracranial hypertension (IIH) is a clinical syndrome of unknown etiology characterized by increased intracranial pressure with normal CSF composition and imaging, which typically affects young, obese women of childbearing age.
IIH is a diagnosis of exclusion that can only be made in patients who satisfy the updated diagnostic criteria [1]. Visual morbidity with subsequent visual field loss is the most feared clinical consequence, which mainly determines the therapy and outcome of the syndrome.
Optical coherence tomography (OCT) is an added tool in the armamentarium for assessing optic nerve head characteristics, such as retinal nerve fibre layer and ganglion cell layer damage, in IIH patients. This non-invasive imaging method of quantitative analysis can help us detect early papilledema. Here, we have analysed the visual manifestations in diagnosed idiopathic intracranial hypertension patients. In the literature, there is only one other Indian study on idiopathic intracranial hypertension patients' characteristics.
2. REVIEW OF LITERATURE
Idiopathic intracranial hypertension (IIH) is a syndrome in which there is increased intracranial pressure of unknown etiology [1]. Various terms have been used to describe this entity. The pseudotumour cerebri syndrome was first described by Quincke in 1897. The most popular and enduring term pseudotumour cerebri was first used in 1914. Foley introduced the term “benign intracranial hypertension” in 1955, which suggests that this disorder is benign, which is misleading as 31% of patients with IIH irreversibly lose vision [2].
The disorder is most commonly termed idiopathic intracranial hypertension after ruling out other etiologies [3]. By definition, IIH includes all patients with isolated raised ICP that is not related to an intracranial process, cerebral venous thrombosis, or meningeal process.
It has been suggested that the terms “primary” and “secondary” intracranial hypertension might be considered to describe IIH further, either 1) the young obese women with isolated raised ICP and no obvious precipitating factors, or 2) patients with isolated raised ICP associated with factors, such as endocrine disorders, anemia, obstructive sleep apnea, medications, or cerebral venous sinus stenosis [4].
At this point, the preferred term “idiopathic intracranial hypertension ” is used and emphasizes the general lack of understanding of the pathophysiology of this disorder.
2.1. Diagnostic Criteria
The diagnostic characteristics of this syndrome were first enumerated by Dandy in 1937 and were later formulated into a set of diagnostic criteria by Smith in 1985 (modified Dandy criteria) (Table 1).
| 1) Signs and symptoms of increased intracranial pressure (headache, nausea, vomiting, transient obscurations of vision, papilledema). |
| 2) No localizing neurological signs otherwise, with the single exception being unilateral or bilateral sixth nerve paresis. |
| 3) CSF can show increased pressure, but no cytological or chemical abnormalities otherwise. |
| 4) Normal to small symmetric ventricles must be demonstrated (originally requiring ventriculography but now demonstrated by CT) |
The modified Dandy criteria do not include advances in neuroimaging technology (Table 2).
| 1) If symptoms present, they may also reflect those of generalized intracranial hypertension or papilledema. |
| 2) If signs present, they may only reflect those of generalized intracranial hypertension or papilledema. |
| 3) Documented elevated intracranial pressure measured in the lateral decubitus position. |
| 4) Normal CSF composition. |
| 5) No evidence of hydrocephalus, mass, structural, or vascular lesion on MRI or contrast-enhanced CT for typical patients, and MRI and MR venography for all others. |
| 6) No other cause of intracranial hypertension identified. |
The criteria presented here provide updated diagnostic criteria for IIH for purposes of routine patient management and for clinical trials.
2.2. Epidemiology of IIH in the World and India
The incidence of IIH has been quoted by some studies. In the United States, the annual incidence of IIH has been reported to be 0.9 per 100,000 in Iowa and 1.07 per 100,000 in Louisiana [5]. In the United States, for women aged 20-44 years, the incidence is approximately 19 per 100,000 [6]. In India, the annual incidence of IIH is 0.9 per 100,000 persons. In India, among women aged 20-44 years, the incidence is 3.5 per 100,000 in those who are 10% more than their ideal body weight [7].
2.3. Risk factors of IIH
2.3.1. Age
The common age of presentation of IIH is between 20-40 years. Despite a high predilection for obese young women, IIH can also occur in children, older adults, and in non-obese persons of either sex [8]. IIH does occur in childhood, but no large epidemiologic studies in this age group have been reported to date. The disorder is rare in pre-pubertal children and has distinct characteristics from the adult form, like stiff neck, diplopia, and strabismus as the commonest presenting symptom. In this age group, papilloedema and strabismus resolve rapidly with medical treatment, and there is no apparent predilection for obese girls [9]. In older teenagers with IIH, however, the rate of obesity is similar to that in the adult IIH population.
2.3.2. Sex
IIH has a higher predilection in women [10]. In a recent large series, the prevalence of IIH in men was approximately 10%, confirming that IIH in men is rare [11].
2.3.3. Obesity
Body mass index (BMI) is a value derived from the weight and height of an individual. It is calculated by dividing the square of height by body mass. BMI ranges for IIH are as follows: underweight <18.5 kg/m2, normal weight 18.5 to 25 kg/m2, overweight 25 to 30 kg/m2, and obese > 30kg/m2. It is typically seen in young women with a body mass index of >25 kg/m2 and in non-obese persons of either sex [12]. Obese women with IIH might have a preferential accumulation of fat in the lower body relative to other obese women in the same age range [13]. In a recent multicenter case-control study of newly-diagnosed women with IIH compared to women who were newly diagnosed with other neuro-ophthalmologic disorders, it was confirmed that higher body mass index is associated with a greater risk of IIH [14]. Another study showed that even non-obese patients were at greater risk for IIH if they had a recent moderate weight gain [15]. Thus, it is likely that the prevalence of IIH in the developed world will rise in parallel with that of obesity [6]. Affected men have a similar body mass index when compared to affected women, but they are, on average, about a decade older than women at the time of presentation [16].
2.3.4. Medications
The use of certain medications can predispose to IIH, such as oral contraceptives, steroids, vitamin A, isotretinoin, lithium, growth hormone, nitrofurantoin, phenytoin, sulfa drugs, minocycline, tamoxifen, naladixic acid, thyroid replacement, tetracycline, and some chemotherapeutic drugs [17].
2.3.5. Anemia
In 2009, a study showed an association between iron deficiency anemia and IIH [18]. The authors have recommended all patients presenting with IIH to have full blood counts, and if they are found to be anemic, they should be treated.
2.3.6. Sleep Disorders
Sleep-related breathing problems have been found to be common in patients with IIH. Obesity is an important risk factor among this group and, therefore, suggests a causative role [19].
2.4. Presentation of IIH
IIH is a disorder defined by clinical criteria and includes symptoms and signs, which are attributed to raised intracranial pressure.
2.5. Symptomatology
The most common symptoms of IIH are as follows:
- Headache - It is present in 92% of cases, and is the most common presenting symptom [20].
- Transient visual obscurations - This symptom is found in 72% of cases, precipitated by a change in position.
- Intracranial noises-pulsatile tinnitus - This symptom is reported in 60% of cases [21].
- Photopsia - It is present in 54% of cases, precipitated by position change and Valsalva.
- Retrobulbar pain - It is found in 44% of cases.
- Diplopia - This symptom has been reported in 38% of cases as intermittent or continuous horizontal diplopia.
- Sustained visual loss - This symptom is present in 26% of cases.
2.6. Headache
This is the most common presenting symptom of IIH [22]. It is of unusual severity, and lateralized, throbbing and pulsatile in character. Wall M, in his study on headache profile in patients of idiopathic intracranial hypertension, described that headaches are often exacerbated by a change in posture, and the pain follows a trigeminal or cervical root distribution with neck stiffness [23]. Rarely do patients present without a headache. Grace et al. studied the characteristics of IIH in prepubertal children in which 29% of children with IIH did not have a headache [9]. In one large case series, men were less likely to complain of a headache than women [16].
2.7. Transient Visual Obscurations (TVO)
TVOs occur in about two-thirds of patients with papilledema, and last seconds at a time [24]. These can be unilateral or bilateral, precipitated by a change in posture, usually sitting, bending over, or lying down or gaze-evoked. Thompson et al. studied visual loss in IIH and found that transient visual obscurations do not appear to correlate with the degree of intracranial pressure elevation or extent of disc swelling and are not predictive of visual loss [25]. TVOs are thought to occur due to transient ischemia of the swollen optic nerve head [26].
2.8. Photopsia
Patients describe photopsia as seeing brief sparkles or flashes of light. Wall et al. conducted a case-control study on symptoms of IIH, which showed that photopsia could be provoked by positional change and Valsalva [27].
2.9. Intracranial Noise
Pulsatile tinnitus is common in IIH. Patients describe hearing the sound of rushing water or wind [6].
2.10. Diplopia
Patients experience intermittent or continuous horizontal diplopia. It can be due to unilateral or bilateral sixth nerve palsy from raised intracranial pressure.
2.11. Ophthalmologic Findings of Idiopathic Intracranial Hypertension
2.11.1. Papilloedema
Papilloedema is the hallmark sign of idiopathic intracranial hypertension [3]. It is typically bilateral and symmteric. It may also be asymmetric. In one series by Chari, Rao on benign intracranial hypertension and its unusual manifestations, 10% of 478 IIH patients had asymmetric papilloedema with more visual loss in the eye with a higher grade of papilloedema [20]. Such patients may also have a relative afferent pupillary defect. Papilloedema can be graded in severity. Frisen scale is used for staging papilloedema.
2.12. Stages Of Papilledema
2.12.1. Normal Optic Disc (Frisen Stage 0)
Stereoscopic viewing of a normal optic disc often reveals mild nasal elevation of the nerve fiber layer. This is due to the increased density of nerve fiber representing the temporal visual field. With the direct ophthalmoscope, the nasal disc margin may appear indistinct compared to the temporal disc rim. The vessels are generally seen coursing across the optic nerve head, although rarely, a portion of a major vessel may be obscured in the upper pole.
2.12.2. Very Early Papilledema (Frisen Stage 1)
The early phase of papilledema consists of the incipient disc changes that occur before the development of obvious disc swelling. Papilledema may be difficult to detect at this stage. During this stage, there may be disruption of the normal radial nerve fiber layer with greyish opacity making the nerve fibre more prominent. A subtle grayish halo may be visible with the indirect ophthalmoscope. In eyes with early papilledema, the peripapillary retina loses its superficial linear and curvilinear light reflexes and appears deep red and without luster. The absence of spontaneous retinal venous pulsations is thought by some investigators to be an early sign of papilledema. According to several authors, pulsations cease when ICP exceeds about 200 mm of water. Thus, if spontaneous venous pulsations are present, ICP should be below this figure. Marked fluctuations in ICP can occur in patients with increased ICP [28-30], and in such patients, the ICP may occasionally drop into the normal range. In addition, spontaneous venous pulsations occur in only about 80% of normal subjects [30]. Thus, 20% of patients with normal ICP also lack spontaneous venous pulsations. For these reasons, the absence of spontaneous venous pulsations does not always support a diagnosis of papilledema. The observation of spontaneous venous pulsations suggests only that the ICP is probably below 200-250 mm of water at that moment.
2.12.3. Early Papilledema (Frisen Stage 2)
Early papilledema is characterized by obscuration of the optic disc borders, elevation of the nasal border, and a complete peripapillary halo. Using stereoscopic color photography and fluorescein angiography, Hayreh and Hayreh concluded that the first sign of raised ICP is swelling of the optic disc [31, 32]. Slit lamp biomicroscopy is especially helpful in this circumstance.“Blurring of the disc margins” is a nebulous description that is neither specific nor helpful. Interpretation of a “blurred” disc margin is often impossible using the direct ophthalmoscope. Unless it is accompanied by other more definitive signs of papilledema, this sign has limited clinical utility.
2.12.4. Moderate Papilledema (Frisen Stage 3)
The optic disc margin becomes obscured and elevated. The diameter of the optic nerve head increases, but the optic cup may still be preserved at this stage. An important finding is the edematous, opaque nerve fiber layer that obscures one or more segments of major blood vessels leaving the disc [32].
2.12.5. Marked Papilledema (Frisen Stage 4)
Marked papilledema shows raised optic nerve head. The optic cup is obscured. There is obscuration of all the borders of the nerve with a marked peripapillary halo. Edema and infarction of the nerve fiber layer cause total obscuration on the disc of a segment of a major blood vessel.
2.13. Other Signs of Papilledema
Other signs of papilledema are as follows:
(1) Flame-shaped nerve fiber layer hemorrhages may increase in number as the ICP increases.
(2) There are cotton wool spots (focal retinal infarcts) with tortuous vessels surrounding the disc.
(3) Severe cases show circumferential retinal folds (Paton’s lines) with linear or curvilinear choroidal folds. The choroidal folds from increased intracranial pressure result in acquired hyperopia [33].
Hard exudates and hemorrhages may occur in the peripapillary region and in the macula, producing decreased central vision [23, 34]. Because nerve fibers in the macula have a radial orientation, hemorrhages and exudates in this region can assume a fan or star shape. Since vascular compromise on and around the optic disc is responsible for these macular changes, the star figure in such cases is usually asymmetric, being more prominent on the nasal side of the fovea toward the disc. Hemorrhages are frequently present with papilledema, although they are not incorporated into the Frisen staging system. Nerve fiber layer hemorrhages are the most common and indicate that the edema is acute to subacute. Such hemorrhages may break into the vitreous in a few cases [35]. This can cause a painless, sudden decrease in vision.
There are some reports of IIH without papilloedema [36]. These patients typically present with intractable headaches and are diagnosed with IIH after an elevated opening pressure is documented on lumbar puncture. The absence of papilloedema is a rare occurrence in IIH. Such patients are not at risk for vision loss.
2.13.1. Visual Loss
Loss of vision is the major morbidity in IIH and may be present on initial evaluation. Visual loss may be gradual but can be abrupt. Visual acuity is less than 20/20 in 10-29% of patients on presentation [24]. Visual acuity is not a sensitive parameter of vision loss in IIH. Vision field loss occurs before a loss of acuity; confrontation visual fields are abnormal in approximately 32% at presentation [37]. Perimetry gives a more definitive assessment of visual field abnormalities. In addition to chronic papilloedema, other mechanisms, such as a serous retinal detachment and subhyaloid hemorrhage, may produce visual loss.
The permanent visual failure was found to affect a third of all children in the non-headache group, but it was rare in children presenting with headaches, with one patient registered blind and two severely visually impaired [38]. Recent reviews have cited a prevalence of functional visual loss (FVL) ranging from 5% to 12% of patients who present with visual loss to a neuro-ophthalmologist. Visual loss in IIH may also arise from macular hemorrhages, exudates, pigment epithelial changes, retinal striae, choroidal folds, subretinal neovascularisation or retinal vascular occlusion.
2.13.2. Abducens Palsy
The sixth nerve palsy may be unilateral or bilateral in patients with IIH [36].
2.13.3. Other Cranial Nerve Deficits
Oculomotor nerve, trochlear nerve, trigeminal nerve, facial nerve, and auditory nerve palsies have been noted in case reports [20].
2.14. Investigations
2.14.1. Visual Field Testing
Visual field testing is very important in assessing the amount of optic nerve involvement in patients with IIH, especially to monitor their response to treatment. Computer-assisted static perimetry is done nowadays. Goldmann kinetic perimetry was done earlier [39].
Enlargement of physiologic blind spot is the earliest visual field defect to occur, and it is a refractive scotoma resulting from the elevation of the peripapillary retina [40]. Severe visual field constriction and inferonasal field defect are other common field changes [26]. Less frequently, central, arcuate, paracentral, and altitudinal scotomas can occur. Central visual field defects occur in IIH patients with longstanding severe papilloedema, but they can sometimes develop rapidly and be present early in the course of the disease [1]. The frequency of visual field loss and acuity loss with IIH is somewhat variable. In one case series, Goldmann perimetry was abnormal in at least one eye in 96% of patients on the initial evaluation [41].
2.15. Confocal Scanning Tomography
It is a type of testing that provides a quantitative measure of papilloedema, and has been shown to correlate with CSF opening pressure and with visual field sensitivity losses and recovery with treatment. While this technique may prove clinically useful, it is not widely available, nor is it clear that it offers significant clinical information over perimetry [42].
2.16. Optical Coherence Tomography
Optical coherence tomography (OCT) is a rapidly evolving technology that has profoundly changed the practice of ophthalmology. Optical coherence tomography (OCT) is a non-invasive imaging method that creates in vivo cross-sectional patterns on the retina and optic nerve head.
Spectral-domain OCT (SD-OCT) increases axial resolution 2- to 3-folds and scan speed 60 to 110-folds in comparison to time-domain OCT (TD-OCT). SD-OCT enables novel scanning, denser sampling, and 3-dimensional imaging [43]. In recent years, OCT has become a valuable tool for assessing retinal axonal damage in several neurological diseases [44].
The retinal nerve fibre layer (RNFL) is composed predominantly of unmyelinated axons of retinal ganglion cells. Measurements of the RNFL should, therefore, give relatively direct measures of the number of axons present.
2.17. Normal Average and Quadrant RNFL Values
Ramakrishnan et al., in 2006, studied retinal nerve fiber layer thickness by optical coherence tomography in the normal Indian population. They studied 118 eyes, which showed mean + standard deviation of retinal nerve fiber layer thickness for various quadrants of inferior, superior, temporal, and nasal, and the entire circumference around the optic nerve head as 138.2 + 21.74, 129.1 + 25.67, 85.71 + 21, 66.38 + 17.37, and 104.8 + 38.81 µm, respectively [43].
Some authors demonstrated characteristics of OCT in IIH patients. Rebolleda et al. compared RNFL thickness measured using Stratus OCT of 22 IIH patients with 22 control subjects, which showed that RNFL thickness correlated with visual field sensitivity losses, and RNFL thickness was found to be 74.9% greater in the IIH group of patients with mild papilloedema [45]. Ophir et al. found thicker RNFL in patients with IIH and papilloedema [24]. This was not supported by a recent study by Falko et al. using spectral domain OCT as it did not show a difference in peripapillary RNFL thickness between controls and IIH patients [46].
In a study on newer perspectives in Neuro-ophthalmology by Gema et al. [10], RNFL thickness measurements were useful for lower grades of papilledema as an adjunct procedure for quantifying disc swelling; however, moderate to severe grades of papilledema yielded inaccurate values of RNFL thickness and GCL analysis by OCT, which were measured by taking the sum of the ganglion cell layer and inner plexiform layer; this may be suitable for early detection of neuronal loss and for identifying patients needing more aggressive treatment.
In a study by Michael et al., peripapillary RNFL measurements correlated with the clinical appearance of the optic discs, suggesting that OCT may assist in the follow-up of IIH patients [47]. Falko et al. suggested SDOCT as a potential diagnostic and progression marker in IIH and other disorders with increased ICP and as a fast and easy diagnostic alternative to repeated lumbar punctures, and could, therefore, ease monitoring of treatment or disease progression [48].
2.18. Neuroimaging
Brain imaging is a must for every patient of IIH as other causes of raised ICP need to be excluded, such as mass lesions, hydrocephalus, and cerebral venous thrombosis, in order to make the diagnosis of IIH.
Certain abnormalities suggestive of raised ICP in IIH seen on MRI are as follows:-
(1) Flattening of the posterior sclera;
(2) Distension of perioptic subarachnoid space;
(3) Enhancement with gadolinium of the prelaminar optic nerve;
(4) Empty sella;
(5) Intraocular protrusion of prelaminar optic nerve;
(6) Vertical tortuosity of the orbital optic nerve.
Imaging of the cerebral venous system with MR or CT venography should be routinely obtained, as it is most sensitive to exclude cerebral venous thrombosis in patients with presumed IIH, especially in men, non-obese patients, children, older patients, and those with an atypical or fulminant presentation, such as trigeminal neuralgia, neck pain, radiculopathy, and facial diplegia, and those with very high CSF opening pressure (>54 cm of water) [49]. There are many reports of cerebral venous abnormalities, such as transverse sinus stenosis, on MRV in patients with IIH.
2.18.1. Lumbar Puncture
Documented elevated intracranial pressure measured in the patient in lateral decubitus position with legs extended is required for diagnosing IIH [50]. The CSF opening pressure should be greater than 250 mm of water. Values between 200 and 250 mm of water are non-diagnostic [50]. Because CSF pressures naturally fluctuate, a repeat lumbar puncture may be necessary if the opening pressure is low in patients with features suggestive of IIH. With CSF opening pressures, on average, 540 mm of water is seen in fulminant IIH cases.
If the neuroimaging study reveals no structural etiology for intracranial hypertension, a lumbar puncture should be performed. In addition to measuring the opening pressure, the CSF composition should be analysed for cell count, differential glucose, and protein. There should be no evidence of pleocytosis, cellular atypia, or hypoglycorrhachia. The CSF protein should be within normal limits [51].
2.19. Treatment
The two goals of treatment in IIH are to alleviate unpleasant symptoms, such as headache, and to preserve vision. Performing a lumbar puncture has a two-fold advantage: not only does it help in diagnosis, but it also decreases the intracranial pressure, although only temporarily. Thus, the treatment itself begins with the diagnostic lumbar puncture, which is often effective in transiently improving symptoms and signs.
2.20. Weight Loss
Weight loss is routinely advised for obese IIH patients. A modest degree of weight loss (about 5-10% of total body weight) is usually required for improvement in symptoms and signs [52].
2.21. Medical Management
Carbonic anhydrase inhibitors, such as acetazolamide, are the main medical treatment prescribed for IIH. They are thought to exert their therapeutic effect by decreasing CSF production, although they also have a mild diuretic effect. Doses of 1-2g daily, given in divided doses, can be effective, although many patients cannot tolerate high doses due to intolerable side effects, such as paresthesias, altered taste sensation, and lethargy, but luckily, the side effects are less as these patients are otherwise well compromised with normal electrolytes and renal function [26].
Steroids have been used as a treatment for IIH in the past, but are associated with significant long-term side effects, such as weight gain, which are undesirable in this patient population. High-dose intravenous steroids are still occasionally used in patients with rapidly progressive visual loss from fulminant IIH, while a more definitive treatment is awaited [36].
2.22. Surgical Procedures
Optic nerve sheath fenestration (ONSF) is advised in patients with papilledema who have marked visual loss, but minimal or absent headache, while in those with visual loss, headache, and papilledema, it is preferred for a CSF diversion procedure, such as ventriculo- or lumbo-peritoneal shunting.
2.23. Optic Nerve Sheath Fenestration
In ONSF, the dural sheath surrounding the retrolaminar portion of the optic nerve is fenestrated, creating a fistula between the subarachnoid space and the orbital cavity [54]. Consequently, there is a reduction in pressure on the optic nerve, leading to reduced papilledema and improved visual function in that eye [34]. The papilledema tends not to recur, although the mechanism for this remains uncertain.
2.24. CSF Shunting Procedures
CSF shunting produces a rapid reduction in ICP, often with a subsequent improvement in symptoms and signs. Lumboperitoneal shunting is more commonly performed than ventriculoperitoneal shunting because insertion and mainte-nance of patency may be more difficult in the latter procedure. The revision rate for lumboperitoneal shunt ranges from 38 to 64%, with an overall revision rate of 52%. The reported interval between shunt placement and first revision is 9-27 months [50].
Our study reports assessment findings in ophthalmological manifestations, including RNFL and GCL assessment using SDOCT in diagnosed patients with idiopathic intracranial hypertension.
3. MATERIALS AND METHODS
3.1. Setting
The study was conducted at the Department of Ophthalmology, Amrita Institute of Medical Sciences, on an Out Patient (OP) basis, on all diagnosed cases of Idiopathic Intracranial Hypertension referred from the Neurology department at the same hospital who met the inclusion/exclusion criteria. They were diagnosed as IIH based on updated diagnostic criteria.
3.4. Exclusion Criteria
Exclusion criteria were as follows:
- Patients with raised intracranial tension due to coexisting illness that can affect ICT.
- Co-existing disease, which can affect the peripapillary RNFL thickness and visual field.
- Patient too ill to allow testing.
3.5. Research Tool
The primary methods used in the study are as follows:
- Proforma;
- Clinical examination;
- Recording of ophthalmological parameters.
All the IIH patients referred from the Department of Neurology were diagnosed by the following:
- Measurement of CSF opening pressure and CSF composition
- Imaging (MRI, MRV/MRA) to rule out other causes for raised ICP
A detailed history, including of headache, transient obscuration of vision, photophobia, tinnitus, phonophobia, nausea, and vomiting, was taken for every patient. All patients underwent a thorough ophthalmology check-up, including
1) Visual acuity, color vision;
2) Intraocular pressure;
3) Extraocular movements;
4) Slit lamp biomicroscopy;
5) Pupil assessment;
6) Stereoscopic examination of the optic disc with 90 Diopter (D) lens on slit lamp;
7) Diplopia charting;
8) Automated perimetry 30-2 and 60-4; and
9) SD-OCT (Zeiss) - Average peripapillary RNFL and GCL thickness assessment.
Using the Fast RNFL mode on the Spectral Domain OCT, Average RNFL measurements of both eyes were taken. Also, average GCL measurements of both eyes were taken. Three readings were taken, and the best one was taken as the measurement. A minimum of 8 as signal strength was taken. We included all patients who satisfied the inclusion criteria in our study.
3.6. Sample Size
The four important study variables are as follows:
1) Visual acuity;
2) Visual field;
3) Nerve fiber layer thickness and ganglion cell layer thickness; and
4) Extra-ocular movements.
The most important of them is the visual field. Based on the result observed from the earlier publications with respect to this variable in IIH patients and with 95% confidence and 20% allowable error, the minimum sample size was taken as 60 patients. However, due to the time limitations of the study period, only 30 patients could be included.
3.7. Statistical Analysis
The percentage of cases with different abnormalities in idiopathic intracranial hypertension patients was assessed. To test the statistical significance of the different ophthalmic abnormalities in idiopathic intracranial hypertension patients, chi-square test with a correction factor was applied. The results obtained will help us in generating a hypothesis with respect to the different types of ophthalmic abnormalities in IIH patients.
3.8. Observations
3.8.1. Study Population
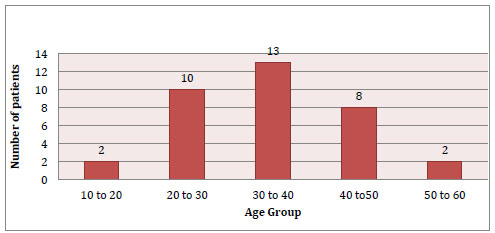
There were a total of 70 eyes of 35 IIH patients selected in our study. Among these IIH patients, 5.71% belonged to the 10-20 age group, 28.57% belonged to the 20-30 age group, 37.14% belonged to the 30-40 age group, 22.85% belonged to the 40 - 50 age group, and 5.71% belonged to the 50 - 60 age group. The highest distribution was in the younger age group, which is in concordance with the characteristic age distribution in IIH. The age-wise distribution of the patients is given in Fig. (1) and Table 3.
|
Age Group (yrs) |
No of Patients(n=35) |
Percentage of Patients |
| 10-20 | 2 | 5.71 |
| 21-30 | 10 | 28.5 |
| 31-40 | 13 | 37.14 |
| 41-50 | 8 | 22.85 |
| >50 | 2 | 5.71 |
3.8.3. Symptoms in the Study Population
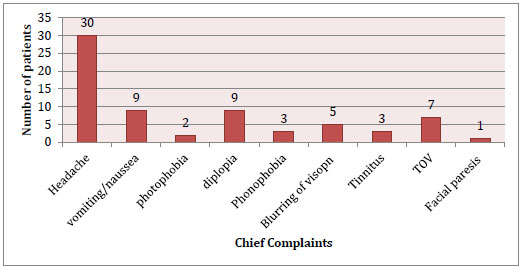
On evaluation, all patients of IIH were symptomatic, out of which 85.7% of patients had a throbbing type of headache as the chief complaint, 25.71% of patients complained of nausea/vomiting and diplopia as the second commonest complaint, while 20% [55] of patients had transient obscuration of vision that lasted for approximately 2-3 mins. There were 14.28% of patients who complained of minimal blurring of vision. The least common complaints were tinnitus (8.57%), phonophobia (8.57%), photobhobia (5.71%), and one patient had right facial paraesis (Fig. 3).
3.8.4. Visual Acuity in the Study Population
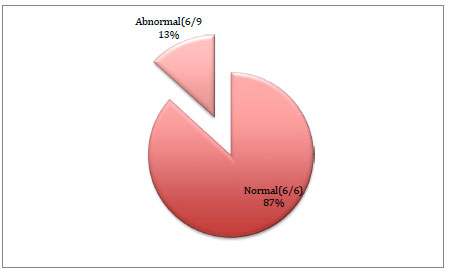
On evaluation, 87% [51] eyes had the best corrected visual acuity (BCVA) of 6/6 on Snellen’s visual acuity chart for distance, and only 13% eyes had BCVA of 6/9 for distance (Fig. 4).
3.8.5. Extraocular Movement Analysis in the Study Population
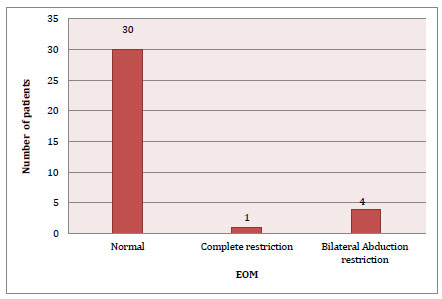
On evaluation, 85.7% [36] patients had normal extraocular movements, 11.42% had bilateral abduction restriction, and one patient had complete restriction of ocular movements (Fig. 5 and Table 4).
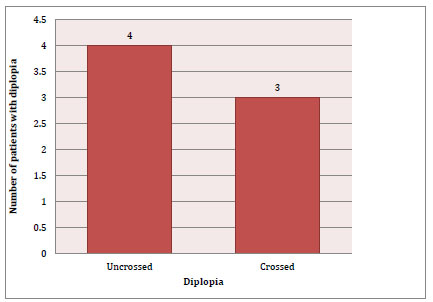
3.8.6. Assessment of Diplopia in the Study Population
On evaluation, 20% [36] patients had diplopia on assessment, out of which 4 (11.4%) patients had uncrossed diplopia (Fig. 6).
Table 4.
| Extraocular Movement |
Patients (n=35) |
Percentage |
| Normal | 30 | 85.7 |
| Bilateral abduction restriction | 4 | 11.4 |
| Bilateral complete restriction | 1 | 2.85 |

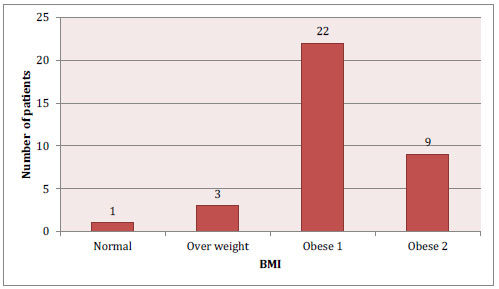
3.8.7. Assessment of Body Mass Index in the Study Population
On evaluation, 2.85% had normal BMI, 8.5% were overweight, 62.8% patients were Obese class I, which was the highest, 25.7% were Obese class II, and none were in the Obese class III group (Fig. 7 and Table 5).
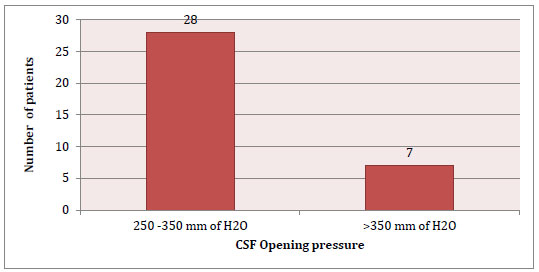
3.8.8. Assessment of CSF Opening Pressure in the Study Population
On evaluation, all 35 patients had elevated CSF opening pressure (>250 mm of water), out of which 80% showed pressures between 250-350mm of water and 20% showed pressures > 350 mm of water (Fig. 8).
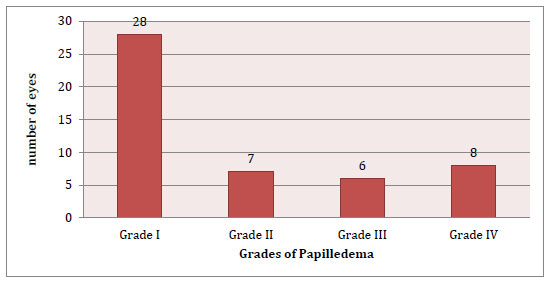
3.8.9. Assessment of Grade of Papilledema in the Study Population
On evaluation, 80% eyes had grade 1 papilledema on assessment, 10% had grade 2 papilledema, 8.5% had grade 3 papilledema, and 11.4% had grade 4 papilledema (Fig. 9 and Table 6).
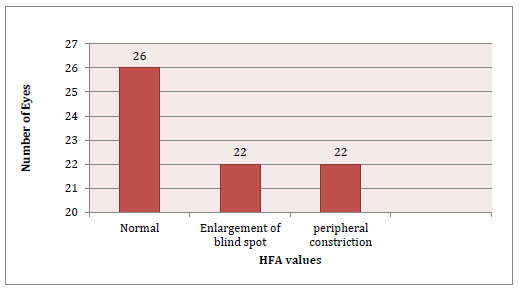
3.8.10. Assessment of Visual Field Changes in the Study Population
On evaluation, 62.85% eyes showed visual field changes on assessment, i.e., 31.4% eyes showed enlargement of blindspot, and a similar percentage of eyes showed peripheral constriction of visual fields. 37.14% showed normal fields (Fig. 10 and Table 7). 12 patients had mean deviation (MD) and pattern standard deviation (PSD) in the normal range. 12 patients had MD < -2, 20 patients had MD less than -6, and 3 patients had MD > -6.
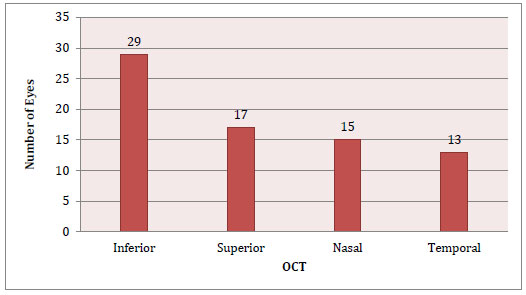
3.8.11. Assessment of Peripapillary Retinal Nerve Fibre Layer Thickness by Spectral Domain Optical Coherence Tomography in the Study Population
On evaluation, 41.4% of eyes showed inferior quadrant retinal nerve fibre layer thickness on SD-OCT, which was the most commonest involved quadrant on assessment. 48.57% of eyes showed superior quadrant retinal nerve fibre layer thickness, 42.85% of eyes showed nasal quadrant retinal nerve fibre layer thickness, and 37.14% of eyes showed temporal quadrant RNFL thickness (Fig. 11).
3.9. Assessment of VEP
VEP was done in 5 patients, out of which 3 showed normal study and 2 patients showed prolonged latency with normal amplitude.
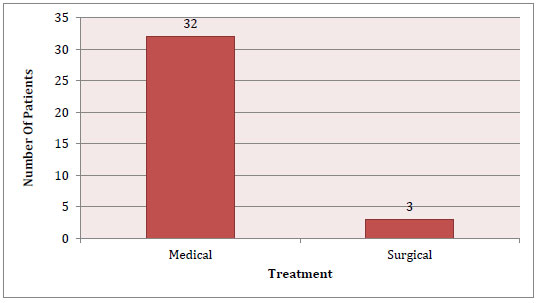
3.10. Assessment of Treatment in the Study Population
On evaluation, 91.4% patients were medically managed and 8.5% underwent surgical treatment. Out of the 3 patients, 2 patients underwent LP shunt and 1 patient underwent VP shunt (Fig. 12).
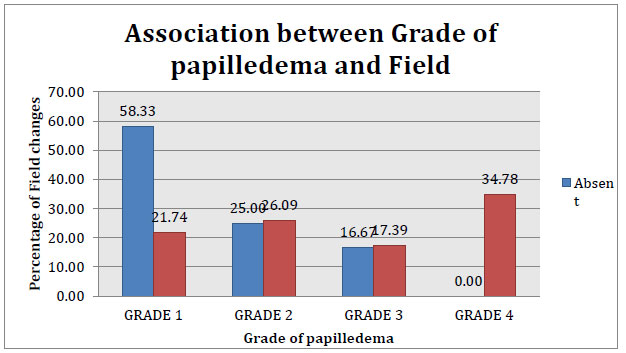
3.11. Grade of Papilledema and its Different Associations
(1) Association of Grade of papilloedema with visual field change (Table 8 and Fig. 13).
A statistically significant association was found between the grade of papilloedema and visual field change with a p-value of 0.06.
2) Association of grade of papilloedema with retinal nerve fibre layer thickness by OCT in the right eye (Table 9) and left eye (Table 10).
No statistically significant association was found between the grade of papilloedema and the retinal nerve fibre thickness in both eyes.
(1) Association of grade of papilloedema with ganglion cell layer thinning by OCT in the right eye (Table 11) and left eye (Table 12).
Table 5.
| BMI | Patients(n=35) | Percentage |
| Normal (18.5 - 24.99) | 1 | 2.85 |
| Over weight (25 - 29.99) | 3 | 8.5 |
| Obese Class I (30 - 34.99) | 22 | 62.8 |
| Obese Class II (35 - 39.99) | 9 | 25.7 |
| Obese Class III (>40) | 0 | 0 |
| Grade of Papilledema |
No. of Eyes (n=70) |
Percentage |
| Grade I | 28 | 80 |
| Grade II | 7 | 10 |
| Grade III | 6 | 8.5 |
| Grade IV | 8 | 11.4 |
| Visual Field Changes |
No. of Eyes (n=70) |
Percentage |
| Normal | 26 | 37.14 |
| Enlargement of blindspot | 22 | 31.4 |
| Peripheral constriction | 22 | 31.4 |
| Visual Field Change | Grade of Papilledema | p-value | |||
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | 0.06 | |
| Absent (13) | 7 (58.3) | 3 (25) | 2 (16.7) | 0 (0) | |
| Present (22) | 5 (21.7) | 6 (26.1) | 4 (17.4) | 8 (34.8) | |
| RNFL Thicknening Right Eye | Grade of Papilloedema | p-value | |||
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | 0.3 | |
| Absent (19) | 9 (47.4) | 4 (21.1) | 2 (10.5) | 4 (21.1) | |
| Present (16) | 3 (18.8) | 5 (31.2) | 4 (25) | 4 (25) | |
| RNFL Thickening Left Eye | Grade of Papilledema | p-value | |||
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | 0.7 | |
| Absent (19) | 7 (43.8) | 4 (25) | 2 (12.5) | 3 (18.8) | |
| Present (16) | 5 (26.3) | 5 (26.3) | 4 (21.1) | 5 (26.3) | |
| GCL Thinning Right Eye | Grade of Papilloedema | p-value | |||
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | 0.8 | |
| Absent (21) | 6 (28.6) | 6 (28.6) | 4 (19) | 5 (23.8) | |
| Present (14) | 6 (42.9) | 3 (21.4) | 2 (14.3) | 3 (21.4) | |
| GCL Thinning Left Eye | Grade of Papilloedema | p-value | |||
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | 0.3 | |
| Absent (21) | 5(23.8) | 6(28.6) | 5(23.8) | 5(23.8) | |
| Present (14) | 7(50) | 3(21.4) | 1(7.1) | 3(21.4) | |
No statistically significant association was found between the grade of papilloedema and ganglion cell layer thinning in both eyes.
3.12. Visual Field Defect and its Different Associations
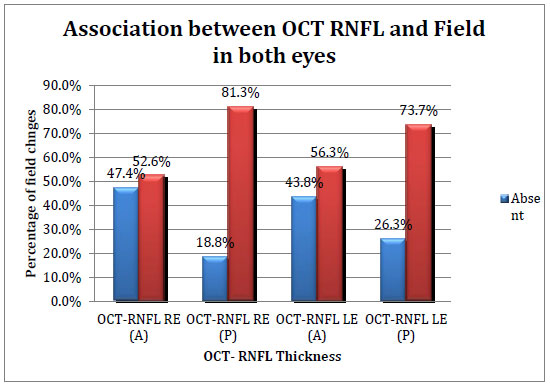
(1) Association of visual field defect with retinal nerve fibre layer thickness in the right eye (Table 13) and left eye (Table 14); Fig. (14) represents this in both eyes.
Even though the patients with the presence of visual field defect showed retinal nerve fibre layer thickening on OCT, no statistically significant association was found in both eyes.
(1) Association of visual field defect with ganglion cell layer thinning by OCT (Tables 15 and 16).
No statistically significant association was found between visual field defect and ganglion cell layer thinning by OCT in both eyes.
Table 13.
| RNFL Thickness Right Eye | Visual Field Defect | p-value | |
| Absent | Present | 0.152 | |
| Absent (19) | 9 (47.4) | 10 (52.6) | |
| Present (16) | 3 (18.8) | 13 (81.3) | |
| RNFL Thickness Left Eye | Visual Field Defect | p-value | |
| Absent | Present | 0.311 | |
| Absent (19) | 7 (43.8) | 9 (56.2) | |
| Present (16) | 5 (26.3) | 14 (73.7) | |
| Ganglion Cell Layer Thinning Right Eye | Visual Field Defect | p-value | |
| Absent | Present | 0.282 | |
| Absent (21) | 9 (42.9) | 12 (57.1) | |
| Present (14) | 3 (21.4) | 11 (78.6) | |
| Ganglion Cell Layer Thinning Left Eye | Visual Field Defect | p-value | |
| Absent | Present | 0.721 | |
| Absent (21) | 8 (38.1) | 4 (28.6) | |
| Present (14) | 13 (61.9) | 10 (71.4) | |
4. RESULTS AND DISCUSSION
Our study consisted of IIH patients who were diagnosed at the Neurology Department based on updated diagnostic criteria. We evaluated various ophthalmic parameters and demographics of these patients. The visual acuity, visual field, grade of papilloedema, RNFL and GCL thickness, and BMI were assessed and correlated in view of finding associations between these parameters.
Idiopathic intracranial hypertension occurs commonly in the younger age group (20-40 years). In our study, the mean age of 35 patients was 34.8 years. Another study done on Indians by Ambika et al. showed mean age of 32.8 years [56]. There were no pediatric patients in our study. We included 31 women and 4 males in our study. There was predominance of women, with a male-to-female ratio of 1:4; this is in concordance with studies by Bruce et al. and Ambika et al., which showed female predominance in the IIH population. Men showed atypical presentations with a lesser incidence of headache.
The patients in our study had a high BMI in Obese Class I (BMI 30-34.99 kg/m). These patients belonging to the Obese class I did not have distinctive clinical presentations. A study on the update of IIH has shown a recent increase in body weight as a risk factor, and another study demonstrated those having IIH to show lower body adiposity [13].
Headache has been described as the most common symptom of IIH. Wall M, in his study, demonstrated that the headache is exaggerated by a change in posture, and pain follows a trigeminal or cervical root distribution with neck stiffness [19]. Rarely do patients present without headache, especially in prepubertal children, as studied by Grace et al. [9], and in men, as studied by Bruce et al. The most common symptom experienced by patients in our study was a throbbing type of headache. Diplopia and nausea/vomiting were the next commonest, which was found to be in accordance with the findings of other studies. Tinnitus, photophobia, and phonophobia were seen in very few patients.
Central visual acuity was well preserved in the majority of our patients. Their best corrected visual acuity was 6/6 on Snellen’s visual acuity chart for distance. Patients with visual loss had only a line drop in visual acuity. This is in contrast to other studies where the visual loss was more [57]. The only other Indian study published in a reputed journal, i.e., a study done on Indian patients of Sankara Nethralaya, showed similar results in visual acuity.
Apart from 4 patients who had bilateral abduction restriction and one patient with sixth and third nerve paraesis, all other patients (n=30) had normal extraocular movements. Most common cause for extraocular movement restriction is abducens nerve palsy, which can be unilateral or bilateral. Oculomotor nerve, trochlear nerve, trigeminal nerve, facial nerve, and auditory nerve palsies have been noted in case reports. These may be more common in prepubertal children than in older patients.
A 44-year-old male patient had complete restriction of all extraocular movements except for depression in adduction with grade 1-2 relative afferent pupillary defect and moderate ptosis. This implies third and sixth nerve paresis with pupil involvement. This was an unusual presentation, which could be attributed to the sex of the patient.
Our patients were proven to be IIH by elevated CSF opening pressure measured by performing a lumbar puncture. Previous studies have shown a positive correlation as the higher the CSF opening pressure, the more the severity of papilledema. However, this was not seen in our study.
All our patients had bilateral papilledema, although in literature, unilateral/asymmetric papilledema has been reported. 80% of our patients showed grade 1 papilloedema using Frisen grading. There are some reports of IIH without papilloedema [58]. These patients typically present with intractable headaches and are diagnosed with IIH after an elevated opening pressure is documented on lumbar puncture. The absence of papilloedema is a rare occurrence in IIH. Such patients are not at risk for vision loss. There was no such patient in our study.
The study by Rowe and Sarkes showed 84% of patients to have visual field defect, and our study demonstrated 62.85% of patients with visual field defects as enlargement of blindspot and peripheral constriction of fields [59]. IIH patients usually do not present a peripheral field dysfunction. Enlargement of physiologic blind spot is the earliest visual field defect to occur, and it is a refractive scotoma resulting from the elevation of the peripapillary retina.
Severe visual field constriction and inferonasal field defect are other common field changes.
None of our patients had an arcuate nasal step. The mean deviation and pattern standard deviation showed a moderate range in 20 patients and severity in 3 patients. Rowe and Sarkie analysed 35 IIH patients prospectively and found visual field assessment as a sensitive indicator of visual loss with a statistically greater sensitivity than visual acuity.
Twenty patients in our study showed RNFL thickening on SD-OCT, with 82.85% of patients showing inferior quadrant RNFL thickening. Rebolleda et al. studied RNFL thickness and found 74.9% greater thickness in the IIH group of patients with mild papilloedema. Ophir et al. found thicker RNFL in patients with IIH and papilloedema.
We found, in our study, a statistically significant association between the grade of papilloedema and the visual field changes, which makes the visual field a reliable investigation in patients with subtle papilloedema. As the severity of papilledema increased, the presence of the visual field increased, implying that it is severe papilledema that leads to visual loss in patients with papilledema. This is an objective finding that patients usually do not perceive.
In our study, RNFL thickness on SDOCT (Zeiss) was compared with the grade of papilloedema, and it showed no correlation. This is consistent with a recent study by Falko et al. using spectral domain OCT, which did not show a difference in peripapillary RNFL thickness between controls and IIH patients. Since this may be due to the fact that we do not know the baseline RNFL thickness prior to the development of papilledema in these patients, although it is seen clinically. In a study by Gema et al., RNFL thickness measurements showed to be useful for lower grades of papilloedema as an adjunct procedure for quantifying disc swelling; however, for moderate to severe grades of papilloedema, OCT yielded inaccurate values of RNFL thickness. Even though the patients in our study with the presence of visual field defect showed retinal nerve fibre layer thickening on SD-OCT, no statistically significant association was found in both eyes.
This is the first Indian study in which RNFL thickness was assessed, but it did not show any positive correlation. Ganglion cell layer has become the most recent adjuvant to assessing optic nerve head dysfunction. More detailed studies need to be done in this aspect. In our study, we found no correlation between ganglion cell layer thinning and the grade of papilloedema. We also found no correlation between ganglion cell layer thinning and visual field changes.
A follow-up of these patients and their OCT characteristics may throw further light on the usefulness of GCC and RNFL parameters in patients of IIH and correlate it with their visual field loss.
CONCLUSION
In our study, all patients had papilledema clinically, with well-preserved central vision. Visual field defects were found on examination, which showed a positive correlation with the severity of papilledema, showing the visual field to be a sensitive indicator. In addition, contrary to expectation, an increase in RNFL on OCT was not a universal finding in our patients in spite of clinically observable papilledema. Furthermore, GCC thinning in these patients needs to be further evaluated with regard to its significance.
LIST OF ABBREVIATIONS
| IIH | = Idiopathic Intracranial Hypertension |
| OCT | = Optical Coherence Tomography |
| TVO | = Transient Visual Obscurations |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study has been approved by the Human Research Ethics Committee (HREC) (Approval no. AIMS-13/15757).
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the human procedures used were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
A written informed consent form was obtained from the patients.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The source of data and materials are what I have collected from the patients by providing them with a questionnaire.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

