All published articles of this journal are available on ScienceDirect.

Clinical-surgical Characteristics of Patients with Macular Hole. Exilaser Ophthalmological Center. Cuenca, Ecuador. 2015-2019
Authors Info & Affiliations
Abstract
Background:
The macular hole (MH) is one of the least studied ophthalmological pathologies; satisfactory treatment has been achieved through the implementation of surgical techniques a few years ago and the study and analysis of its clinical-surgical characteristics are of vital importance to assess the success of surgery with intrinsic and extrinsic factors.
Objective:
Describe the clinical-surgical characteristics of patients diagnosed with a macular hole at the EXILASER Ophthalmological Center in Cuenca in the period 2015-2019.
Methods:
Descriptive, retrospective study. The study universe corresponds to 75 patients who attended the EXILASER Ophthalmological Center and were diagnosed with MH between January-2015 and December-2019.
Results:
76.0% of the patients are women; 81.3% are between 60 and 79 years old; 96.0% reside in urban areas; 34.7% are dedicated to housework; 24.0% report cataracts; 26.7% have arterial hypertension; 84.0% presented loss of central vision; 80.0% had decreased visual acuity. 50.7% presented affection only in the right eye; 53.3% had a chronic evolution greater than one year; 33.3% presented grade III MH. 44.0% had surgery; 93.9% had anatomical surgical closure. The relationship between the degree of MH, time of evolution, and closure of the MH was not significant (p> 0.05).
Conclusion:
The success rate of MH closure after surgical intervention is greater than 90% with improvement in postoperative visual acuity. No significant association was found between the grade of the MH, time of evolution, and the closure of the MH.
1. INTRODUCTION
Idiopathic macular hole, or simply macular hole, is a rare retinal disease that affects older people, particularly women. Macular holes can be seen in very nearsighted eyes or after ocular trauma, but the vast majority are idiopathic. The ocular macula is a small region located inside the retina and plays a very important role in the visual process, since it allows us to
distinguish shapes, objects, and colors, considering that sight is one of the most important senses for human beings in the performance of their daily activities. Likewise, the macula is of utmost importance since it is responsible for central vision, by processing the images perceived by the eye and sending them to the brain.
In 2018, Tarib et al. reported a clinical case in Morocco, where a 67-year-old male patient was referred for an acute decrease in visual acuity in his left eye and diagnosed with idiopathic stage IV MH; 3 weeks after the operation, the patient complained of a decrease in visual acuity limited to hand movement, which would fall within the statistics that state that 3 to 6% of cases of MH at this stage do not require surgery; the follow-up of the case was performed by optical coherence tomography (OCT) [1].
Castro and Gonzalez [2] in 2003, performed a study in 50 eyes of 48 patients where they experimentally proved the advantages of performing the liberation of the limiting membrane in the surgery of MH, due to the fact that there was an anatomical recovery of 100% of the cases, besides a slight percentage of recovery of the visual acuity in the studied patients.
Ramos and collaborators in 2016, determined some of the factors that accompany idiopathic MH and that can be considered good prognosis for anatomical and functional recovery; within them, it is observed that patients with less time of evolution, in stage II or less and a hole smaller than 400 microns have a greater recovery in terms of anatomy and function, after the surgery performed [3].
In a study conducted in 2016 by Guerrero, it was determined that surgical success for MH surgery is higher than 10% considered as a success factor in the recovery of visual acuity; which in general lines increased significantly in the cases studied, they were people between 60 and 75 years of age with an improvement ranging from 0.05 to 0.3 on average [4].
Lizana and collaborators in 2008, establish anatomical and functional results after MH surgery of 59 eyes of 54 patients, where it was concluded that postoperative visual acuity was superior to preoperative, also the difference in proportions of MH closure with and without limitorrhexis was statistically significant in favor of vitrectomy without limitorrhexis [5].
In 2018, Brito et al. conducted a study in Mexico City, where they evaluate two treatment schemes for MH closure, such as exoplant and vitrectomy, finding that for the study population, there are no significant differences between the anatomical and functional success of each technique applied, but only the early detection of this pathology determines the postoperative improvement [6].
The authors agree that the significant deterioration of central vision is the biggest problem and the main sign described by the patient who comes to the ophthalmology office prior to the diagnosis of MH, being also the most important parameter, together with the anatomical repair that is evaluated at the moment of determining the success of a treatment or the spontaneous closure of the MH, the latter, especially in early stages of the pathology [7-9].
The MH was first described by Knapp in Germany in 1869 and was commonly associated with a pathology of difficult management since a specific treatment was not clear; in the last decades the analysis of this disease has regained special interest, due to the fact that studies of some of the etiological factors, the physiopathogenesis in general and the correct treatment have proven to be very effective [7, 8, 10].
The main problem in treating MH was that it was believed that the photoreceptors located in the fovea were completely destroyed when the pathology occurred, whether idiopathic or non-idiopathic, until 1991, when new vitreoretinal surgery techniques were developed, including vitrectomy; Thus, Kelly and Wendel performed vitrectomy for the first time in Minnesota - United States in 1991, releasing the posterior hyaloid and fluid-gas exchange, observing a total success both in the anatomical and functional recovery of the patient's MH that was operated [11].
Nowadays, each case of MH is well analyzed, looking for the causes and the best treatment option, where the surgery called vitrectomy is optimal and timely in most cases, in patients there is a great diversity in the clinical and surgical characteristics of this entity [10, 11].
According to The Baltimore Eye Study, for the year 2001, the worldwide prevalence would be 3.3 per 1,000 inhabitants; it is not a subject that has been studied very much, so we do not have specific epidemiological data for our country or for others (13). It is more frequent after 55 years of age, specifically between 65 and 74 years, and between 10 and 15% develop MH in the contralateral eye with a higher incidence in women than in men, with a 3:1 ratio [12-15].
This population is studied in Cuenca, Ecuador, at the private Exilaser Ophthalmologic Center, which serves the ophthalmologic patient population. This facility generates information about the history and variables related to the pathology of MH that can be used to understand its behavior and to make an updated and pertinent description of the disease.
The causes of MH are diverse, although it has been shown that the disease itself is not among the most common visual conditions, the damage it causes to the patient's quality of life and the degenerative characteristics observed require health professionals to provide timely help.
As it is a disease that does not have a defined origin, it is very important to make a previous analysis of the causes that could trigger the presence of this nosological entity, to report if it is of idiopathic origin, and to describe the main clinical and surgical characteristics of each patient, since the properties of the lesion, its degree, the patient's visual acuity, the rapid establishment of surgical treatment, differ according to the origin of the lesion; it is not possible to study separately the MH, the etiology and the characteristics of each patient [13-16].
In addition, in Ecuador there have been no recent studies on this disease, while those that exist are very superficial; the subject is little studied, so it is not known with certainty what are the variables related to MH, which opens the opportunity to develop research on the subject and know what are the family history, age groups, sex, the degree of impairment of visual acuity without correction and with correction that are more frequent in Cuenca. On the other hand, there are few academic publications that have studied in depth the signs and symptoms with which patients with MH present in our environment, as well as the degrees of the staging of the disease and the relationship of these degrees with the closure of MH post-surgery, which is the surgical success of the same.
For this reason, a question arises:
What are the clinical-surgical characteristics of patients with MH in the Exilaser ophthalmologic center of Cuenca in the period 2015-2019?
The relevance of this research project is considered due to the need to have accurate, systematized, structured, and organized data on the main clinical and surgical characteristics of patients with MH of different origins in the Exilaser ophthalmologic center of the city of Cuenca-Ecuador; the analysis of these data will give us valuable and truthful information of the pathology under study.
This study benefits patients who have lost their vision due to this disease; It also contributes to the medical community in the area of ophthalmology in Ecuador to have access to updated information on the clinical-surgical characteristics of MH, which will contribute to the early diagnosis of the disease and optimal management of patients, as well as to improve the treatment of the disease, since 20 years ago it was considered incurable, it is pertinent to make an approach to the new advances in diagnostic techniques, such as optical coherence tomography, in addition to all the technology and surgical implements used worldwide at present, the fact that there are few investigations on this subject worldwide and especially in our country, which has been superficial and basic, confirms the justification of the current research.
The study was carried out at the Exilaser Ophthalmologic Center because it attends a large number of patients from the Austro region with retinal diseases, specifically with MH since it has human personnel with a subspecialty in the retina and state-of-the-art technology for the diagnosis and surgical treatment of this pathology.
2. OBJECTIVES
2.1. General Objective
To describe the clinical-surgical characteristics of patients with MH seen at the Centro Oftalmológico Exilaser de Cuenca during the period 2015-2019.
2.2. Specific Objectives
- To distribute the sample according to: age, sex, place of origin, occupational occupation.
- Identify family and personal, systemic, and ophthalmologic history.
- Determine the main symptoms and signs of the affected patients.
- Classify patients according to the degree of corrected and uncorrected, preoperative, and postoperative visual acuity.
- Relate the degree of MH and the time of evolution of MH to the surgical outcome.
3. METHODOLOGICAL DESIGN
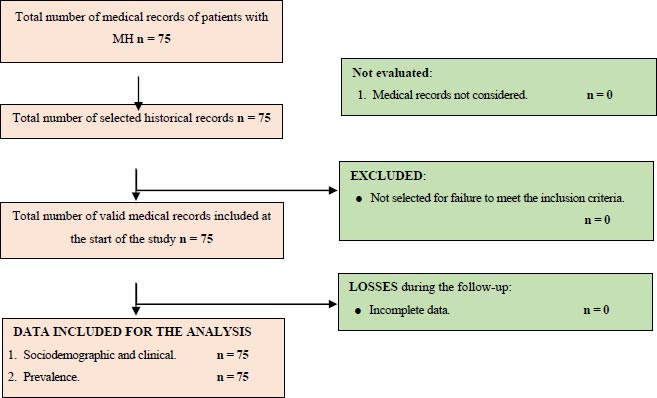
The study is descriptive, retrospective, and cross-sectional. For the development of the present study, different variables were analyzed: sex, age, occupation, origin, ophthalmologic personal history, ophthalmologic family history, systemic personal history, systemic family history, signs, symptoms, visual acuity without correction, visual acuity with correction, degree of MH, time of evolution, surgical outcome. The universe is constituted by all the medical records of patients who have attended the Exilaser Ophthalmology Center and have been diagnosed with MH, during the period from January 2015 to December 2019. We worked with the universe, a total: of 75 patients (Fig. 1).
It was performed at the Centro Oftalmológico Exilaser located in the city of Cuenca.
- Inclusion criteria were:
- (1) Complete clinical histories of patients who attended the Exilaser ophthalmologic center and were diagnosed with MH during the period from January 2015 to December 2019.
- Exclusion criteria for the present study were:
- (2) Incomplete medical records.
The medical records of patients with MH during the period 2015-2019 were reviewed. Data collection was based on the retrospective method and was carried out using a clinical record designed for the study, in which the required data were copied from the observation of the clinical history; the data were copied faithfully to what was written in each clinical history so that all the necessary information for the development of the present investigation was observed in a clear, separate and orderly manner.
The data were collected in situ from the clinical records of the Exilaser Ophthalmological Center in the city of Cuenca, Ecuador, with the necessary permission to access the information as well as the appropriate COVID-19 biosafety material in times of pandemic to carry out this process.
Once the cards were completed, the data were transcribed into a matrix made in an MS-Excel spreadsheet, where each column corresponded to a variable and each row to the complete record of a card. This matrix was filled in by the researchers, who took into account the inclusion and exclusion criteria, as well as not leaving blank spaces or omissions.
In the case of the 4 patients with bilateral MH, the eye where the condition began was selected for the study. The method was carried out by means of documentary observation of clinical histories of the selected universe and in the technique the data were taken from the clinical histories of each patient from the file cabinet of the Exilaser Ophthalmologic Center. In this research, a form designed by the researchers with variables to be studied was used for data collection.
All the information collected for the proposed study was handled with absolute confidentiality and the data obtained were used only for research purposes; the record of each patient was coded numerically so that the patient cannot be identified in the record or in the database. Likewise, at no time can the patient be identified, since the data were statistically processed and are presented in aggregate form of frequencies and percentages. Once the titer score has been obtained, the files will be destroyed.
The authors of the study declare that they have no conflicts of interest.
Data tabulation was performed in a data matrix designed in the Microsoft Excel program of the Office 2016 package; from there, the data were exported to the SPSS version 25 statistical software, where the statistical processing was performed through the elaboration of frequency tables and percentages, which were used in tables in order to allow their rapid comprehension.
The association analysis was carried out using contingency tables and the Chi-square statistic, under a significance level of 0.05; the null hypothesis of the hypothesis contrast establishes the independence between the variables, while the alternative hypothesis indicates the significant association between the variables; thus if the p-value is less than 0.05, it is concluded that the relationship between the variables is significant.
| Variable | Category | Frequency | Percentage |
| Sex | Female | 57 | 76.0% |
| Male | 18 | 24.0% | |
| Age | Under 60 | 9 | 12.0% |
| 60-64 | 22 | 29.3% | |
| 65-69 | 25 | 33.3% | |
| 70-74 | 14 | 18.7% | |
| 75-79 | 2 | 2.7% | |
| Over 80 | 3 | 4.0% | |
| Origin (type of residence) | Urban | 72 | 96.0% |
| Rural | 3 | 4.0% | |
| Ocupation | Housewife | 26 | 34.7% |
| Retired | 24 | 32.0% | |
| Worker | 22 | 29.3% | |
| Student | 3 | 4.0% | |
| Total | 75 | 100.0% | |
As the information was obtained from the institution's medical records, we did not work directly with patients in the study (consent is not applicable). The research was approved by the Ethics Committee of the Exilaser Ophthalmologic Center, agreement #3, Act 4, year 2023, code 2023-04-03.
4. RESULTS
According to Table 1, of the 75 patients participating in the study, 76.0% are female and 24.0% are male. 33.3% of the patients are aged between 65 and 69 years, 29.3% are aged 60 to 64 years and 18.7% belong to the 70 to 74 years age group; therefore, patients aged 60 to 79 years accumulate 81.3% of the total number of participants.
With respect to origin, 96.0% reside in urban areas and 4.0% in rural areas. Of the total number of patients in the sample, 34.7% were engaged in household chores, 32.0% were retired, 29.3% were working and 4.0% were students.
Regarding personal ophthalmologic history, 24.0% of patients report cataracts, 10.7% have myopia, 9.3% have pterygium, 8.0% have conjunctivitis and 6.7% have astigmatism, these being the main antecedents. On the other hand, 30.7% of the patients had no personal ophthalmologic history (Table 2).
Regarding ophthalmologic family history, 12.0% of patients report diabetic retinopathy and 5.3% cataracts, being those with the highest frequency. On the other hand, 61.3% of the patients had no ophthalmologic family history (Table 3).
As the main personal systemic antecedents found in the study, it was obtained that 26.7% have arterial hypertension, 20.0% have diabetes mellitus, 9.3% have rheumatism, 9.3% have hypercholesterolemia, and another 9.3% have thyroid disorders. Of the total number of patients, 26.7% reported no personal systemic history. Presentation and analysis of data and results (Table 4).
| Personal Ophthalmologic History | Frequency | Percentage |
| Cataract | 18 | 24.0% |
| Myopia | 8 | 10.7% |
| Pterygium | 7 | 9.3% |
| Conjunctivitis | 6 | 8.0% |
| Astigmatism | 5 | 6.7% |
| Retinal detachment | 3 | 4.0% |
| Hypermetrope | 3 | 4.0% |
| Stye | 3 | 4.0% |
| Diabetic retinopathy | 3 | 4.0% |
| Glaucoma | 2 | 2.7% |
| Strabismus | 1 | 1.3% |
| Presbyopia | 1 | 1.3% |
| Amaurosis | 1 | 1.3% |
| does not refer | 23 | 30.7% |
| Ophthalmologic Family History | Frequency | Percentage |
| Diabetic Retinopathy | 9 | 12.0% |
| Cataract | 4 | 5.3% |
| Retinal detachment | 3 | 4.0% |
| Glaucoma | 3 | 4.0% |
| Myopia | 3 | 4.0% |
| Amaurosis | 3 | 4.0% |
| Astigmatism | 2 | 2.7% |
| Strabismus | 2 | 2.7% |
| Hypermetrope | 2 | 2.7% |
| Presbyopia | 2 | 2.7% |
| Pterygium | 2 | 2.7% |
| Conjuntivitis | 1 | 1.3% |
| Stye | 1 | 1.3% |
| Does not refer | 46 | 61.3% |
| Personal Systemic History | Frequency | Percentage |
| Arterial hypertension | 20 | 26.7% |
| Mellitus diabetes | 15 | 20.0% |
| Rheumatism | 7 | 9.3% |
| Hypercholesterolemia | 7 | 9.3% |
| thyroid disorders | 7 | 9.3% |
| Depression | 5 | 6.7% |
| Cancer | 2 | 2.7% |
| Chronic obstructive pulmonary disease | 2 | 2.7% |
| Heart failure | 2 | 2.7% |
| Systemic lupus erythematosus | 2 | 2.7% |
| Cerebrovascular disease | 2 | 2.7% |
| Chronic renal insufficiency | 1 | 1.3% |
| Coagulation disorders | 1 | 1.3% |
| does not refer | 20 | 26.7% |
| Systemic Family History | Frequency | Percentage |
| Mellitus diabetes | 29 | 38.7% |
| Arterial hypertension | 23 | 30.7% |
| Cancer | 7 | 9.3% |
| thyroid disorders | 6 | 8.0% |
| COPD | 4 | 5.3% |
| Rheumatism | 4 | 5.3% |
| Hypercholesterolemia | 3 | 4.0% |
| Depression | 3 | 4.0% |
| Chronic renal insufficiency | 3 | 4.0% |
| Heart failure | 2 | 2.7% |
| Systemic lupus erythematosus | 2 | 2.7% |
| Coagulation disorders | 2 | 2.7% |
| cerebrovascular disease | 1 | 1.3% |
| does not refer | 11 | 14.7% |
| Signs and Symptoms |
Frequency (N: 75) |
Percentage |
| Loss of central vision | 63 | 84.0% |
| Decreased visual acuity | 60 | 80.0% |
| Black spots in the visual field | 10 | 13.3% |
| Total loss of vision in the affected eye | 10 | 13.3% |
| Metamorphopsia | 9 | 12.0% |
| Foveal depression | 7 | 9.3% |
Among the systemic family history, it was observed that 38.7% of the patients indicate diabetes mellitus, 30.7% arterial hypertension, 9.3% cancer, and 8.0% thyroid disorders. Of the total number of patients, 14.7% reported no systemic family history (Table 5).
Loss of central vision was reported as the most frequent of the signs and symptoms with 84.0%; 80.0% of the patients present decreased visual acuity; 13.3% black spots in the visual field and another 13.3% total loss of vision of the affected eye; finally, metamorphopsia was observed in 12.0% and depression of the fovea in 9.3% of the patients (Table 6).
Regarding uncorrected visual acuity, 32.0% present a record of 20/200, 21.3% of 20/400, and 17.3% count fingers or lower; these being the most frequent (Table 7).
| Uncorrected Visual Acuity | Frequency | Percentage |
| Count fingers or less | 13 | 17.3% |
| 20/400 | 16 | 21.3% |
| 20/200 | 24 | 32.0% |
| 20/100 | 10 | 13.3% |
| 20/80 | 10 | 13.3% |
| 20/60 | 2 | 2.7% |
| Total | 75 | 100.0% |
| Visual Acuity with Correction | Frequency | Percentage |
| Count fingers or less | 9 | 12.0% |
| 20/400 | 14 | 18.7% |
| 20/200 | 9 | 12.0% |
| 20/100 | 15 | 20.0% |
| 20/80 | 10 | 13.3% |
| 20/60 | 9 | 12.0% |
| 20/40 | 7 | 9.3% |
| Mejor de 20/40 | 2 | 2.7% |
| Total | 75 | 100.0% |
| Eye Affected | Frequency | Percentage |
| Right | 38 | 50.7% |
| Left | 33 | 44.0% |
| Both | 4 | 5.3% |
| Total | 75 | 100.0% |
| Time of Evolution | Frequency | Percentage |
| Acute (less than 6 months) | 13 | 17.4% |
| Subacute (6 months to 1 year) | 22 | 29.3% |
| Chronic (greater than 1 year) | 40 | 53.3% |
| Total | 75 | 100.0% |
Regarding visual acuity with correction, 20.0% of patients present a visual acuity of 20/100, 18.7% of 20/400, and 13.3% of 20/80 (Table 8).
Table 9 shows that 50.7% of the patients presented affection only in the right eye, 44.0% in the left eye, and 5.3% in both eyes.
Regarding the time of evolution of the visual pathology, 53.3% have a chronic evolution time greater than one year, 29.3% subacute from 6 months to one year, and 17.4% acute less than 6 months (Table 10).
Table 11 shows 33.3% of patients present grade III of MH, 28.0% grade II, and 24.0% grade IV, these being the most frequent.
Of the total number of patients in the study, 44.0% underwent surgery, while 56.0% did not decide to opt for surgical treatment (Table 12).
Table 11.
| Degree | Frequency | Percentage |
| Degree I | 11 | 14.7% |
| Degree II | 21 | 28.0% |
| Degree III | 25 | 33.3% |
| Degree IV | 18 | 24.0% |
| Total | 75 | 100.0% |
| Surgical Intervention | Frequency | Percentage |
| Yes | 33 | 44.0% |
| No | 42 | 56.0% |
| Total | 75 | 100.0% |
| Affected Eye | Surgical Resolution | Total | |
| Surgical | No Surgical | ||
| Right | 34.2% | 65.8% | 100.0% |
| Left | 54.5% | 45.5% | 100.0% |
| Both | 50.0% | 50.0% | 100.0% |
| Total | 44.0% | 56.0% | 100.0% |
| Surgical Outcome | Frequency | Percentage |
| AM Closing | 31 | 93.9% |
| Do not close the AM | 2 | 6.1% |
| Total | 33 | 100.0% |
| Postoperative Visual Acuity | Frequency | Percentage |
| Count fingers or less | 1 | 3.0% |
| 20/400 | 3 | 9.1% |
| 20/200 | 7 | 21.2% |
| 20/100 | 7 | 21.2% |
| 20/80 | 4 | 12.1% |
| 20/60 | 6 | 18.2% |
| 20/40 | 2 | 6.1% |
| Better than 20/40 | 3 | 9.1% |
| Total | 33 | 100.0% |
It was observed that 34.2% of patients with right eye involvement were surgically intervened, 54.5% of patients with left eye involvement, and 50% with both eyes (Table 13).
Of the total number of operated patients, 93.9% have as a surgical outcome the closure of the MH and 6.1% the non-closure of the MH (Table 14).
In the operated patients, it was observed that 21.2% presented visual acuity of 20/200, as well as another 21.2% an acuity of 20/100; in third place, there were patients with a visual acuity of 18.2% obtained 20/60 after surgery (Tabla 15).
Table 16.
| Grade | Hole Closure | No Hole Closure | Total | |||
| No. | % | No. | % | No. | % | |
| III | 18 | 58.06 | 1 | 50 | 19 | 57.57 |
| IV | 13 | 41.94 | 1 | 50 | `14 | 42.43 |
| Total | 31 | 100 | 2 | 100 | 33 | 100 |
| - | Hole Closing | No Hole Closing | ||
| No. | % | No. | % | |
| Less than 6m | 2 | 6.45 | 0 | 0 |
| From 6m to 1 year | 8 | 25.81 | 1 | 50.0 |
| More than a year | 21 | 67.74 | 1 | 50.0 |
| Total | 31 | 100 | 2 | 100 |
When analyzing the relationship between MH grade and surgical outcome, it was obtained that there are no significant differences due to the change in categories, given that the p-values are greater than 0.05; therefore, MH grade is not significant for surgical outcome (Table 16).
Regarding the relationship between evolution time and surgical outcome, it was obtained that there is no significant association between these variables since the p-values are greater than 0.05; therefore, evolution time does not significantly affect surgical outcome (Table 17).
5. DISCUSSION
MH is a full-thickness round opening in the foveal center; it is a retinal defect located in the center of the fovea, causing significant vision impairment. The primary goal of MH surgery is to close the hole involving pars plana vitrectomy, removal of the posterior and classic hyaloid epiretinal hyaloid membrane, along with the removal of any diaphanous contractile membranes found on the retinal surface [17, 18].
The number of study participants was limited to 75 patients who attended the Centro Ophthalmologic Exilaser de Cuenca during the period 2015-2019, which may be related to the overall low frequency of the disease, in addition to the difficult study and diagnosis; however, by reviewing other studies it can be found that the sample size found in this research is sufficient. Reference can be made to the study conducted by Pinto et al. [19], on a sample of 614 patients with ocular diseases, of which 0.1% presented MH, that is, about 61 patients. On the other hand, in a study conducted in Olmsted County, Minnesota, by McCannel et al. [20], the authors reported that idiopathic macular holes occur with an age- and sex-adjusted frequency of 7.8 persons and 8.69 eyes per 100,000 inhabitants per year.
This result was similar to that found by Pitta et al. [21], who studied a population of 27 eyes of 25 patients with MH in Bandung, Indonesia; 76% were female and 24% were male. Kim et al. [22] conducted an investigation in 26 eyes of 26 patients, where 73.1% of the patients were female, while in the study of Kuo et al. [23], 70.3% of the patients were female. Likewise, in the study by Ramos-López et al. (3), it was observed that 66.7% of the patients were female. McCannel et al. [24] concluded in their study that the ratio of women to men with Mh was 3.3 to 1.
One-third of patients with MH are between 65 and 69 years of age, while the 60 to 79 years age group represents 4 out of every 5 patients. Pitta et al. [21] found that 56% of patients with MH are between 60 and 69 years of age, while Ramos-López et al [3] observed that 50% of patients were between 60 and 64 years of age. As can be seen, the disease is prevalent in adults over 60 years of age, so we agree with the aforementioned studies.
Most of the patients reside in urban areas, which represents almost the totality of the participants in the investigation; meanwhile, one-third of the patients are engaged in household chores. No studies were found that reported the prevalence of patients with MH by area of residence and occupation.
As the most frequent personal history, a quarter of all patients were found to have cataracts, while among the ophthalmologic family history, diabetic retinopathy and cataracts were the most frequent.
In the research conducted by Kuo et al. [23], it was determined that lamellar MH associated with diabetic retinopathy had worse baseline visual acuity, wider defect, and more pronounced parafoveal schists; however, a significant visual improvement could be obtained after the operation.
One out of four patients with MH have arterial hypertension and one out of five have diabetes mellitus; while, among the systemic family history, diabetes mellitus and arterial hypertension prevail. Waluyojati et al. [24] observed that 50% of patients with MH had a history of arterial hypertension and 37.5% had Diabetes Mellitus 2, which are systemic diseases already reported in relation to MH.
Among the signs and symptoms, loss of central vision and decreased visual acuity were reported as the most frequent among patients with MH (4 out of 5 patients). According to Dubón and Mendoza [25], the loss of central vision is a consequence of the damage observed in the macula, which can be aggravated by the presence of risk factors such as arterial hypertension, diabetes mellitus 2, and retinopathies.
Regarding uncorrected visual acuity, one-third of patients have a visual acuity of 20/200, while, regarding corrected visual acuity, one out of five patients have a visual acuity of 20/100.
Half of the patients presented involvement only in the right eye. In the study by Ramos-López et al. [3], 69.1% of the patients had MH in the right eye, which is higher than that found in the present study.
Slightly more than half of the patients with MH have a chronic evolution time of more than one year. In contrast, in the study by Ramos-López et al. [3], 59.5% of patients with MH were found to have an evolution time of less than one year, which is evidence of the delay in clinical diagnosis.
One-third of the patients had grade III MH, being the most frequent. Pitta et al. [21] observed that 78% of patients with MH present grade IV. We consider that the higher frequency of patients with grade III is due to the fact that at this stage the patient becomes aware of the decrease in visual acuity and does not come to the clinic at earlier stages or when he/she has premonitory symptoms.
A little less than half of the total number of patients with MH were operated on; this was due in most cases to the inability to assume the costs of surgery or to the little hope of improvement in visual acuity assumed by the patient. It was also observed that the greatest proportion of surgeries were performed on patients with an affected left eye.
Almost all the patients had surgical outcomes after the closure of the MH. Similarly, in the research of Kim et al. [22], it was observed that 96.2% of the patients showed successful closure of the MH after the primary operation. Ramos-Lopez et al. [3] observed that 85.7% of surgical patients achieved closure of the idiopathic MH. A lower value was found by Pitta et al. [21], with 74% of surgical patients with closed MA and 26% without MH closure after surgery; while in the study by Passarelli et al. [26], anatomical closure of the MH was observed in 72.1% of the patients who underwent surgery. We consider that in the present study, there was surgical success in most of the patients.
Of the patients who underwent surgery, two out of ten had visual acuity of 20/200, while two others reported visual acuity of 20/100. In the study performed by Castro and Gonzalez [2], it was observed that visual acuity was improved in 68% of the total number of eyes that underwent surgery, which was seen in one or more Snellen lines. Regardless of the closure of the hole, in most cases visual acuity is not substantially improved, although it does not reach values as in other ocular surgeries (cataract, refractory myopia), due to the anatomical and functional complexity of the macular tissue. This type of surgery, being successful, does not have such a high visual prognosis, compared to other ocular surgeries, a factor that also influences the non-surgical decision of some patients.
According to León et al. [17], the management of MH is somewhat controversial, since there are two types of treatment, according to the patient's situation: expectant and surgical; in young patients’ expectant management can be performed for a period of six months, depending on the patient's evolution.
In the set of patients in the study, it was found that the degree of MH and the time of evolution do not affect the surgical outcome, since the p-values were greater than 0.05. Therefore, the influence of timely diagnosis on the impact on the retina and the success of the surgery cannot be evidenced; this may be related to the low prevalence of macular holes, which does not allow us to have a large enough sample to observe significant differences.
Few studies were found on the clinical-surgical characteristics of MH; this may be due to the low prevalence of the disease due to its traumatic origin. In this regard, Urías-Planella et al. [27] state that only 1% to 9% of blunt ocular traumas may be accompanied by traumatic MH. However, the literature on the subject shows that the disease is also associated with age, being more frequent in older adults than in early stages of life; according to Montesinos et al. [28], children with MH and other macular disorders respond successfully, and more quickly to surgical interventions, with results of 20/20 visual correction being observed within 9 months.
CONCLUSION
- Regarding sociodemographic variables, we had that patients with MH are predominantly female gender, with a ratio of 3 to 1 with respect to male gender; 8 out of 10 patients with MH are between 60 and 79 years old; most reside in urban areas; and one third are engaged in household chores.
- The most frequent symptoms were loss of central vision and decreased visual acuity which occurred more frequently 20/200 without correction, with more involvement in the right eye.
- Half of the patients with MH have a chronic evolution time greater than one year. One out of every 3 patients have grade III MH.
- The prevalence of surgical interventions in patients with MH was half, and it was evidenced that most of them have a surgical outcome after the closure of the MH with an improvement of postoperative visual acuity.
- No significant differences were found between the grade of the MH and the surgical outcome; neither between the time of evolution and the surgical outcome.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research was approved by the Ethics Committee of the Exilaser Ophthalmologic Center, agreement #3, Act 4, year 2023, and code 2023-04-03.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
As the information was obtained from the institution's medical records, we did not work directly with patients in the study (consent is not applicable).
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author, [E.R], on special request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

