All published articles of this journal are available on ScienceDirect.

A Systematic Review and Meta-analysis of Convergence Insufficiency Prevalence and Management Options
Abstract
Background:
Convergence insufficiency (CI) is one of the most common binocular vision disorders. The condition negatively affects the quality of life through its impact on near activities, while there is a large gap in the information on its global prevalence and consensus on treatment.
Objectives:
The purpose of this systematic review and meta-analysis was to assess the prevalence and treatment options available for convergence insufficiency.
Methods:
The study was performed in 2023 using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-2020) guidelines. The authors have searched Google Scholar, Research Gate, Scopus, PubMed, Index Medicus, Web of Science, and the JAMA network. This review included peer-reviewed studies published between January 2000 to January 2023 that assessed the prevalence and treatment modalities of convergence insufficiency.
Results:
The authors screened 13250 studies, 20 for prevalence and 15 for treatment from 12 countries that met the inclusion criteria for the study. The overall pooled prevalence of convergence insufficiency was 7.98%, and the heterogeneity between the studies was highly significant P < 0.0001. Majorities of the studies 12(80%) reported that office-based vision therapy is the most effective treatment of CI, form those studies 5(42.0%) highlighted that office-based vergence/accommodative therapy with home reinforcement is the best modality of treatment. Whereas, home-based pencil push-up therapy, vision therapy with modified refractive correction, and vision therapy with prismatic correction were reported as effective treatment options for CI. The reviewed studies showed that vision therapy is highly effective to recover from symptomatic CI in both adults and children.
Conclusion:
The prevalence of convergence insufficiency was high, there was highly significant heterogeneity between the reviewed studies. Office-based vergence/accommodative therapy with home reinforcement is the best modality of treatment, followed by home-based pencil push-up therapy, vision therapy with modified refractive correction, and vision therapy with prismatic correction. There is consensus among reviewed studies that vision therapy is highly effective to recover from symptomatic CI in both adults and children.
1. INTRODUCTION
Convergence insufficiency (CI) is one of the most common binocular vision anomalies that cause difficulty in near activities [1, 2]. The condition leads to the discomfort of near vision, and functional difficulties such as reading, writing, and confused attention, resulting in impaired education, poor academic performance, and task achievements [3-5]. CI is typically described as a group of clinical signs that appear at near fixation, such as exophoria, a receded point of convergence, and reduced positive fusional vergence amplitude [6]. Anne et al. reported that the near point of convergence break performed best in detecting children with CI during the school vision screening [7]. A previously published study reported that correction of refractive errors results in the resolution of many vergence and accommodative disorders [8].
Patients suffering from CI commonly complain of asthenopia symptoms such as eyestrain, blurring of vision, diplopia, headaches, and reading difficulties [9-11]. In the United States of America, symptomatic CI is a prevalent binocular vision defect affecting approximately 5% of the population [12, 13]. An early study showed that CI had been confirmed to be a prevalent binocular vision disorder among both children and adults and recommended that there is a critical need for studies to assess it is prevalence among students who learn in a digital setting [14]. Among the studies conducted in various regions with different environments and ethnic backgrounds, the findings showed the prevalence of CI varied between 1.7 to 33% [9]. Whereas, the prevalence of CI among school-aged children reported in the literature varies from 2% to 13% [15]. An earlier study [16] showed that there was no significant difference in the prevalence of CI with age up to 60 years, but it increased significantly after 60 years. Furthermore, similar findings from a study conducted in Iran revealed that the prevalence of CI is affected by age, gender, and refractive condition [17]. In the last decade, the literature showed the CI Symptom Survey (CISS), which is a questionnaire used as an indicator for the treatment of CI, a study conducted in 2015 suggests that the CISS questionnaire is not specific to detect convergence insufficiency [5]. A further study reported that the accurate prevalence of CI in the general population has not been investigated due to the different criteria for its diagnosis [18].
There are several types and modalities for the treatment of CI that can be prescribed, such as base-out prism spectacles, pencil push-ups, vision therapy, and home-based computer vergence/accommodative therapy, there is a lack of information and rareness of unanimity about the most convenient treatment [19, 20]. Maryam and other authors compared the efficiency of three approaches of vision therapy for treating CI, they reported that in adults, office-based vision therapy was more effective than the other options for treatment [19]. The findings from a study performed in South Korea suggest that vision therapy is successful in repose the symptoms of CI [21,22]. Another study was designed to compare the effectiveness of home-based pencil push-ups and office-based vision therapy in emmetropes with CI associated with asthenopia symptoms; the study found no difference between the two methods of therapy [23]. Amit et al, reported that smartphone-based fusion exercises connected with modified glasses prescriptions are more effective in the treatment of symptomatic CI [24]. Previously published studies [25, 26] showed that improvements in reading performance were found after office-based vergence/accommodative therapy. Most of the treatment studies of CI did not report any side effects for any of the earlier techniques, moreover, they showed great adherence to office-based vergence/ accommodative therapy [27, 28]. As mentioned above, there is a large gap in the information on its global prevalence and consensus on the treatment of CI. Therefore, this systematic review and meta-analysis assessed the prevalence and treatment modalities available for CI.
2. MATERIALS AND METHODS
2.1. Strategy and Selection Criteria
The present study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines [29]. The researchers have searched Google Scholar, Research Gate, Scopus, PubMed, Index Medicus, Web of Science, and the JAMA network. This systematic review and meta-analysis included peer-reviewed studies published between January 2000 and January 2023 that assessed CI prevalence and available treatment modalities. In this study, the search keywords were performed using the Boolean operator (OR/AND): The keywords used to search were frequency, incidence, prevalence, rate or proportion, and clinical presentation and treatment of CI.
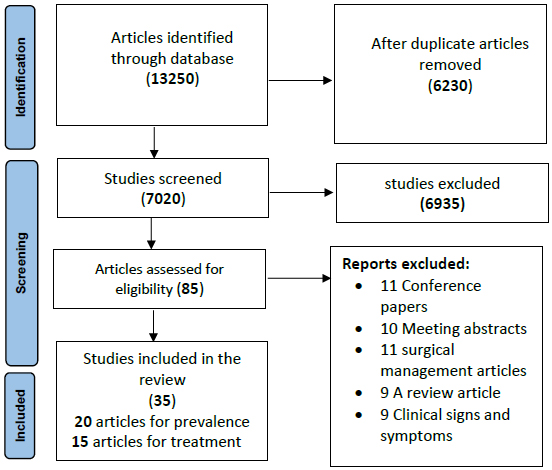
The review was focused on English language articles conducted to assess the prevalence and treatment options for CI taken for all age groups. CI Symptom Survey questionnaire studies were excluded because of the validity and reliability used in the calculation of prevalence, the review articles also were excluded from the calculation and analysis of prevalence. The study also excluded studies without basic data collection, conference papers, meeting abstracts, and editorial discussions. Whereas in the treatment of CI studies, we excluded the studies without basic data collection, as shown in Fig. (1).
2.2. Data Collection and Extraction
The authors evaluated the articles through the titles and abstracts, to investigate the prevalence, the principal investigator extracted the given author’s name, year of publication, country of study, sample size, and age groups. Whereas in the treatment modalities of CI, the principal investigator extracted the data from randomized controlled trials examining any types of non-surgical treatment and comparative studies for all age groups. The types of treatment vary from study to study, such as home-based computer vergence/accommodative therapy, office-based vergence/ accommodative therapy, pencil/target push-ups, base-in prism combined with progressive addition lenses, and placebo therapy. The outcomes of treatment in these studies evaluated depend on near point of convergence, positive fusional vergence, and/or CI Symptom Survey.
2.3. Data Analysis
The data from the inclusive articles were registered independently in a prepared Microsoft Excel Sheet format containing information about the first author’s name, study country, year of publication, means of age, size of samples, and the prevalence and treatment of CI. Then Meta-analysis for the prevalence of CI was performed using MedCalc-Version 19.6.1 software (Mariakerke, Belgium). In the current study, heterogeneity among studies was evaluated by a Q-statistic that is distributed as χ2 under the assumption of homogeneity of effect sizes, and I2 index I2 values ranged between 0 and 75%, representing none to high heterogeneity. Finally, analyzed information was used to create tables presenting the prevalence of CI and the equivalent weight for each study. The overall pooled prevalence of CI was assessed using a random-effect model and its associated 95% confidence intervals (CI). P values less than 0.05 were statistically significant.
3. RESULTS
3.1. Study Characteristics
In this systematic review and meta-analysis, we found 13250 studies, as shown in Fig. (1). When taking away duplicate studies, the authors reviewed the titles of approximately 7020 studies. Formerly, the authors excluded 6935 studies after reading abstracts since they did not meet the inclusion criteria and the aim of the study, and the authors excluded 50 studies after reading their full texts as the essential data cannot be extracted, the total of reviewed studies 35 articles (Fig. 1). The final meta-analysis of the prevalence of CI included 20 studies from 12 countries, as shown in Table 1. Publication years were 2014–2023, and the overall sample size of the studies was 27333 subjects with a mean age of 16.13 ±3.85 years.
| First Author and Year of Study | Country |
Age Mean (Years) |
Age S.d. |
Sample Size |
Study Design | Prevalence of CI (%) |
|---|---|---|---|---|---|---|
| Hashemi 2017 [17] | Iran | 30.50 | 14.00 | 3132 | Cross-sectional | 5.51 |
| Hassan 2017 [30] | Sudan | 15.50 | 2.50 | 4211 | Cross-sectional | 7.8 |
| Nunes 2019 [9] | Portugal | 10.90 | 0.90 | 372 | Cross-sectional | 2 |
| Carla 2022 [31] | Spain | 9.60 | 1.30 | 628 | Cross-sectional | 5.3 |
| Ma 2019 [32] | China | 15.90 | 0.80 | 928 | Cross-sectional | 2.7 |
| Davis 2016 [8] | USA | 11.70 | 1.80 | 484 | Cross-sectional | 6.2 |
| Jang 2015 [33] | South Korea | 10.50 | - | 589 | Cross-sectional | 10.3 |
| Hussaindeen 2017 [34] | India | 12.70 | 2.70 | 920 | Cross-sectional | 17 |
| Li 2020 [35] | China | 9.33 | 0.02 | 4123 | Cross-sectional | 12.4 |
| García-Muñoz 2016 [36] | Spain | 22.90 | 3.69 | 175 | Cross-sectional | 3.43 |
| Singh 2017 [37] | India | 10.00 | - | 4838 | Cross-sectional | 2.79 |
| Jorge 2022 [38] | Portugal | 24.4 | 4.80 | 107 | Cross-sectional | 10.3 |
| Franco 2022 [39] | Portugal | 24.9 | 5.30 | 156 | Cross-sectional | 7.1 |
| Manish 2021 [40] | Nepal | 24.00 | - | 210 | Cross-sectional | 11.42 |
| Darko-Takyi 2016 [41] | Ghana | 22.62 | 1.53 | 105 | Cross-sectional | 1.90 |
| Ovenseri-Ogbomo 2016 [42] | Nigeria | 18.5 | 2.20 | 212 | Cross-sectional | 4.0 |
| Wajuihian 2016 [43] | South Africa | 16.27 | 1.79 | 1201 | Cross-sectional | 4.30 |
| Kim 2023 [44] | South Korea | 8.20 | 7.6 | 5385 | Cross-sectional | 9.40 |
| Sharif 2014 [45] | Iran | 21.70 | 2.80 | 160 | Cross-sectional | 10.00 |
| Vaishali 2019 [46] | India | 26.54 | 17.45 | 142 | Cross-sectional | 27.46 |
| All | - | 16.13 | 3.85 | 27333 | - | 7.98 |
| Authors (Years) | Country | Prevalence (95% CI) | Weight (%) |
|---|---|---|---|
| Hashemi 2017 [17] | Iran | 5.51(5.00-6.00) | 11.15 |
| Hassan 2017 [30] | Sudan | 7.8(7.00-9.00) | 10.86 |
| Nunes 2019 [9] | Portugal | 2(1.00-4.00) | 3.28 |
| Carla 2022 [31] | Spain | 5.3(4.00-7.00) | 2.34 |
| Ma 2019 [32] | China | 2.7(2.00-4.00) | 6.58 |
| Davis 2016 [8] | USA | 6.2(4.00-8.00) | 1.55 |
| Jang 2015 [33] | South Korea | 10.3(8.00-13.00) | 1.18 |
| Hussaindeen 2017 [34] | India | 17(15.00-19.00) | 1.21 |
| Li 2020 [35] | China | 12.4(11.00-13.00) | 7.1 |
| García-Muñoz 2016 [36] | Spain | 3.43(1.00-6.00) | 0.98 |
| Singh 2017 [37] | India | 2.79(2.00-3.00) | 33.14 |
| Jorge 2022 [38] | Portugal | 10.3(5.00-61.00) | 0.22 |
| Franco 2022 [39] | Portugal | 7.1(5.00-6.00) | 0.44 |
| Manish 2021 [40] | Nepal | 11.42(7.00-15.00) | 0.39 |
| Darko-Takyi 2016 [41] | Ghana | 1.90(1.00-2.00) | 1.04 |
| Ovenseri-Ogbomo 2016 [42] | Nigeria | 4.0(2.00-7.00) | 0.97 |
| Wajuihian 2016 [43] | South Africa | 4.30(3.00-5.00) | 5.39 |
| Kim 2023 [44] | South Korea | 9.40(9.00-10.00) | 11.75 |
| Sharif 2014 [45] | Iran | 10.00(5.00-15.00) | 0.33 |
| Vaishali 2019 [46] | India | 27.46(21.00-36.00) | 0.13 |
| All | 7.98(5.00-10.00) | 100.00 | |
| Heterogeneity between groups | P < 0.001 | - | |
| I2 (inconsistency) | 98.41 | - | |
3.2. Prevalence of Convergence Insufficiency Worldwide
A meta-analysis of CI prevalence among subjects with a mean age of 16.13 ±3.85 years is shown in Table 1. The overall pooled prevalence of CI was (7.98%, 95%CI: 5.00-10.00; p<0.001), and almost 40% of reviewed studies (n =8) reported a significantly higher prevalence of CI and 35% (n = 7) reporting the lower prevalence of CI compared with the pooled estimated prevalence. The study conducted by Vaishali et al., 2019 [46] presented the highest CI prevalence of 27.46%(95%CI:21.00-36.00) in Indian people mean aged 26.54± 17.45 years, while Nunes et al, 2019 [9] reported the lowest prevalence among Portuguese children 2% (95%CI:1.00-4.00) their mean aged 10.90±0.9 years. The pooled prevalence estimates of CI in the current study was similar to the study conducted by Hassan et al., 2017 [2], 7.8% (95%CI 7.00-9.00) among secondary school students in Khartoum, Sudan, mean aged 15.50±2.50. There was ex- tremely significant heterogeneity between the studies included in this meta-analysis (P < 0.0001) as shown in Table 2.
3.3. Treatment of Convergence Insufficiency
The authors included 15 trial studies conducted for the treatment of CI, 9 of them conducted in children (less than 18) and 4 in adults (18 to 40 years), with 1641 participants from 15 countries, 1185 of them being children. The publication years between 2005–2022 as shown in Table 3. These clinical trials evaluated and compared these procedures; home-based pencil push-ups (HBPP), office-based orthoptic therapy (OBOT), Smartphone-based exercises in conjunction with modified glasses prescription, vision therapy, home-based computer orthoptic program, placebo vision therapy, office-based placebo therapy with home reinforcement (OBPT) and prismatic correction. The diagnostic measurements and outcomes were comparable among these clinical trials.
| Authors (Years) | Country | Sample | Age | Treatment Outcome |
|---|---|---|---|---|
| Singh 2021 [22] | India | 176 | 22.7 ± 6.84 (A) 21.1 ± 7.2 (B) |
Comparable results between home-based pencil push-up therapy PPT and office-based orthoptic therapy |
| Mohan 2019 [24] | India | 150 | 15 and 30 | Smartphone-based exercises in conjunction with modified glasses prescription are more effective |
| Jang 2017 [21] | South Korea | 235 | 10.13 ± 2.45 | vision therapy is highly effective in the relief of the symptoms |
| Gallaway 2002 [47] | USA | 25 | - | PPT improved both objective findings and symptoms |
| Huston 2015 [48] | USA | 186 | 5 to <18 | Home-based computer vision therapy reduced objective findings and symptoms. |
| Scheiman 2005 [49] | USA | 47 | 9 to 18 | Vision therapy/orthoptic was more effective than pencil push-ups or placebo vision therapy/orthoptics in reducing symptoms and improving objective results |
| CITT 2008 [50] | USA | 221 | 9 to 17 | Office-based vergence/accommodative therapy with home reinforcement results in a significantly greater improvement in symptoms and other objective findings |
| Scheiman. 2009 [51] | USA | 72 | 9 to <18 | The effectiveness of office-based vergence/accommodative therapy was more than home-based or placebo treatment. |
| Scheiman 2005 [52] | USA | 46 | 19 to 30 | Office-based vision therapy/orthoptics was more effective |
| Dusek 2011 [53] | UK | 134 | 7-14 | Highly effectivity for both prismatic correction and home vision therapy. |
| Aletaha 2018 [19] | Iran | 84 | 26.8 ± 8.3 | Effectiveness of office-based orthoptic |
| Scheiman 2010 [54] | - | 221 | 9 to 17 | Office-based vergence/accommodative therapy with home reinforcement is more effective than others. |
| Serna 2011 [55] | USA | 42 | - | Home-based computer orthoptic therapy reduced the symptoms and improved the objective results |
| CITT 2019 [56] | USA | 310 | 9- to 14- | Comparable finding for office-based placebo and office-based vergence/accommodative therapy. |
| Scheiman 2018 [26] | USA | 44 | 9-17 | Office-based vergence/accommodative therapy improved reading skill |
Majorities of the studies 12 (80%) reported that office-based vision therapy is the most effective treatment of CI; from those studies 5(42.0%) highlighted that office-based vergence/ accommodative therapy with home reinforcement is the best modality for the treatment of CI. Whereas, home-based pencil push-up therapy, vision therapy with modified refractive correction, and vision therapy with prismatic correction were reported as effective treatment options for CI. In children, the finding of three studies showed that vision therapy is highly effective to recover from symptomatic CI, followed by accommodative therapy with home reinforcement (OBVAT) and office-based vergence/accommodative. Whereas, in adults, the clinical trials showed the office-based orthoptic treatment was more effective than the other treatments option, as shown in Table 3.
4. DISCUSSION
The findings of the current review provided recent estimates of the convergence insufficiency prevalence and the effective treatment modalities worldwide using data from thirty-five studies from fifteen countries conducted from 2005 to 2022. Our study revealed that the overall pooled prevalence of convergence insufficiency was 7.98%. There was highly significant heterogeneity between the studies P < 0.0001.
As reported in previously published studies, there is a dearth of information on prevalence rates of CI globally, and recommended that more studies are necessary to provide a theory-based CI definition, prevalence, diagnosis, and treatment. More studies of CI will help to establish effective diagnosis and treatment guidelines. In the present, the highest prevalence of CI was reported among Indian adults aged 18-35 years [46] and Indian school-aged children [34], while the significantly lowest CI prevalence was found among Portuguese children [9] and Chinese high school students [32]. Conversely, the study conducted among secondary school students in Sudan [30] shows comparable CI prevalence to the overall estimation. In our review, countries, such as India, showed differences in the prevalence of CI among the different ages at 27.46% [46], 17% [34], and 2.79% [37]. Moreover, studies conducted among Portuguese people reported the lowest prevalence of CI 2% [9], and the highest at 10.3% [38]. Our reviewed studies showed that the prevalence of CI was within the range prevalence 2 to 27.46% in the studies population and a previously published study [57, 58] reported a prevalence range of 1.7 to 33% was found. The variation in CI prevalence within the state and region may be because of different environmental and heredity factors or the norms for defining the condition or measurement methods.
There has been a great deal of uncertainty and debate regarding the management of CI. However, recently, various studies have been conducted to find out the efficiency of some previously known treatment procedures. Regarding the best modality of treatment for CI majority of the reviewed studies showed that office-based vision therapy is the most effective way, particularly vergence/ accommodative therapy with home reinforcement. Whereas, home-based pencil push-up therapy, vision therapy with modified refractive correction, and vision therapy with prismatic correction were reported as effective treatment options for CI. The reviewed studies showed that vision therapy is highly effective in recovering from symptomatic CI in both adults and children. The reviewed studies in children and adults showed that vision therapy is more effective to eliminate the symptoms of convergence insufficiency. This could be due to most patients with CI having weak positive fusional vergence, and most of the vision therapy techniques depend on improving positive fusional vergence amplitude and vergence accommodation relationship. Our findings agreed with Scheiman et al., who reported that office-based vision therapy was a more effective treatment of CI in children [59]. Scheiman et al., suggested that for young adults, outpatient vision therapy is the most effective treatment for CI, in improving positive fusional vergence at near fixation [59]. Moreover, previously published studies [60-62] reported that office-based vergence-accommodative treatment with home enforcement was more effective than other procedures.
5. LIMITATIONS
Our study had some limitations related to it being a review study. These included variations in the study approaches, such as some studies included large sample sizes and different age groups, which may give over or underestimation of CI prevalence. Numerous articles were not included in this study as they used different techniques, reducing the number of studies. In future studies, it is better to use meta-analysis to assess the effect of different treatment modalities for convergence insufficiency. Nevertheless, of these limitations, the current systematic review and meta-analysis estimated the pooled prevalence of CI and the effective treatment modalities.
CONCLUSION
In conclusion, the present review highlights that the prevalence of convergence insufficiency was high, and there was highly significant heterogeneity between the reviewed studies. Regarding CI treatment, office-based vergence/ accommodative therapy with home reinforcement is the best modality of treatment, followed by home-based pencil push-up therapy, vision therapy with modified refractive correction, and vision therapy with prismatic correction. There is consensus among reviewed studies that vision therapy is highly effective to recover from symptomatic CI in both adults and children.
LIST OF ABBREVIATIONS
| CI | = Convergence Insufficiency |
| CISS | = CI Symptom Survey |
| HBPP | = home-based Pencil Push-ups |
| OBOT | = office-based Orthoptic Therapy |
| OBVAT | = office-based Vergence/accommodative |
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS OF REPORTING
The present study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.
SUPPLEMENTARY MATERIAL
PRISMA checklist is available as supplementary material on the publisher’s website along with the published article.

