All published articles of this journal are available on ScienceDirect.

Diversity of Microbial Species Implicated in Keratitis: A Review
Authors Info & Affiliations
Abstract
Background:
Microbial keratitis is an infectious disease of the cornea characterised by inflammation and is considered an ophthalmic emergency requiring immediate attention. While a variety of pathogenic microbes associated with microbial keratitis have been identified, a comprehensive review identifying the diversity of species has not been completed.
Methods:
A search of peer-reviewed publications including case reports and research articles reporting microorganims implicated in keratitis was conducted. Search engines including PubMed, Scopus and Web of Science with years ranging from 1950-2012 were used.
Results:
232 different species from 142 genera, representing 80 families were found to be implicated in microbial keratitis. Fungi exhibited the largest diversity with 144 species from 92 genera. In comparison, 77 species of bacteria from 42 genera, 12 species of protozoa from 4 genera and 4 types of virus were identified as the infectious agents. A comparison of their aetiologies shows reports of similarities between genera.
Conclusions:
The diversity of microbial species implicated in keratitis has not previously been reported and is considerably greater than suggested by incidence studies. Effective treatment is heavily reliant upon correct identification of the responsible microorganisms. Species identification, the risk factors associated with, and pathogenesis of microbial keratitis will allow the development of improved therapies. This review provides a resource for clinicians and researchers to assist in identification and readily source treatment information.
BACKGROUND
Microbial keratitis is an infectious disease of the cornea that is characterised by inflammation, often with stromal infiltration by leukocytes, and is considered an ophthalmic emergency requiring immediate attention. Both infectious and immune mechanisms are important in the development of this sight threatening condition [1, 2]. Keratitis can progress rapidly with corneal destruction through pathological wound healingwithin 24-48 hours [3-5]. A decade-old estimate for keratitis induced corneal ulcers of approximately 2 million per annum in the developed world is likely to be conservative [4]. Permanent visual dysfunction has been reported in a significant number of patients in both developed and developing nations [6].
Initial management of microbial keratitis is empiric with broad-spectrum topical antimicrobials, as with current microbiological investigations it can take days or even weeks to identify a causative organism. This reliance on antimicrobials has been implicated in the emerging resistance in some countries to some of these commonly used antimicrobial agents [7]. Furthermore, topical therapy has limitations, including their rapid loss caused by drainage and high tear turnover and ocular toxicity [8]. Patients with microbial keratitis continue to lose vision and suffer ocular pain and discomfort. Clearly, improved therapies for microbial keratitis are required, while a more rapid and correct identification of the infectious agent supports a more effective treatment.
A variety of pathogenic microbes have been associated with microbial keratitis [9], but to date a comprehensive review of the responsible microbes has not been performed. Identification of the responsible organisms, the risk factors associated with, and pathogenesis of microbial keratitis will allow the development of improved therapies. In this paper we identify and report the diversity of microbial species implicated in keratitis, as well their aetiologies and reported treatments.
METHODS
A systematic review of the current literature pertaining to the identity of organisms implicated in microbial keratitis was conducted. PubMed, Scopus and Web of Science searches were performed using the terms ‘microbial keratitis’, ‘keratitis’, ‘bacterial keratitis’, ‘fungal keratitis’, ‘amoebic keratitis’ and ‘viral keratitis’. Searches were conducted within the year limits for each of the data bases; these were from 1950 for PubMed, 1950 for Scopus and 1950 for Web of Science. Searches were restricted to English Language.
Publications were read and information reporting identification of organisms implicated in microbial keratitis abstracted on the basis of (a) organisms identity, (b) aetiology and (c) treatment. The review objective was restricted to species diversity and did not aim to compile any incidence data.
RESULTS AND DISCUSSION
A range of microorganisms, including fungi, bacteria, protozoa, and viruses, have been identified as infectious agents in microbial keratitis. An exhaustive review of the literature to identify the species diversity revealed 232 different species from 142 genera, representing 80 families, although it is unclear which were opportunistic infections and whether any possess virulence factors that support the initiation of infection. Based on the literature, the greatest diversity of species associated with keratitis is fungal with 144 species from 92 genera. In comparison, 75 species of bacteria from 42 genera, 9 species of protozoa from 4 genera and 4 types of virus have been identified as the infectious agents in microbial keratitis (Fig. 1).
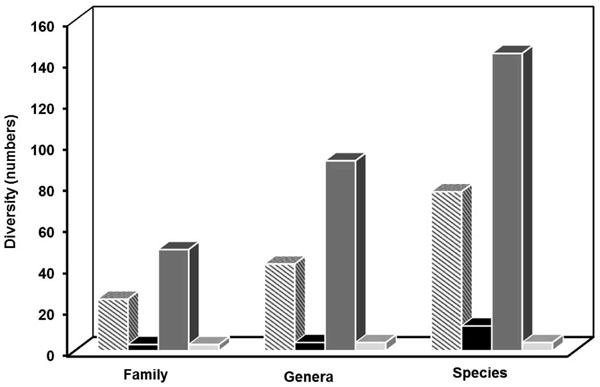
Distribution of microorganisms associated with keratitis, at the family, genera and species levels based on the literature, amoebic ■, bacterial ■, viral and fungal keratitis .
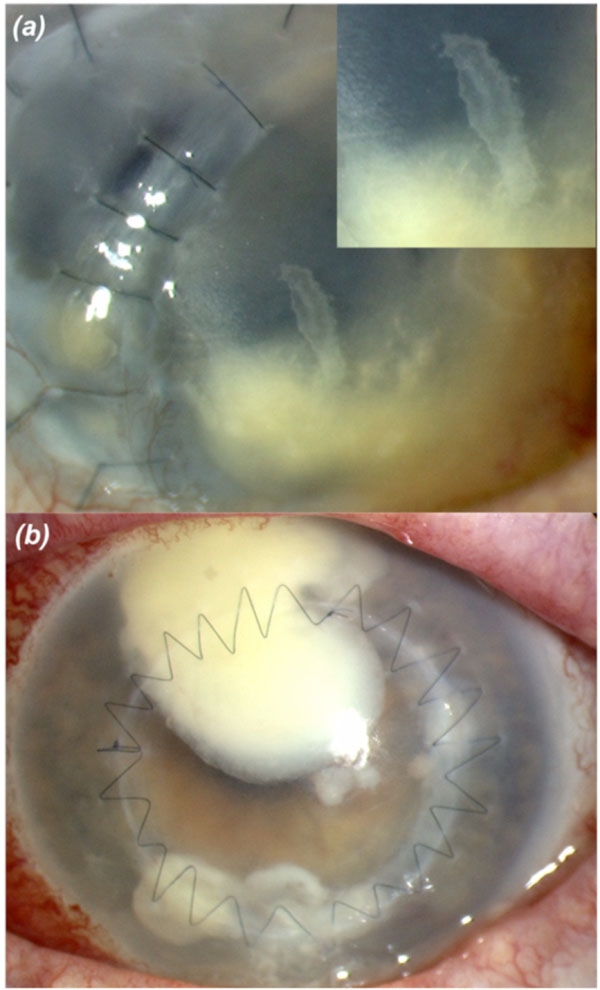
Mycotic keratitis following corneal grafting with (a) filamentary, Aspergillus, Insert: higher magnification showing the irregular feathery margins, and (b) unicellular, Candida spp.
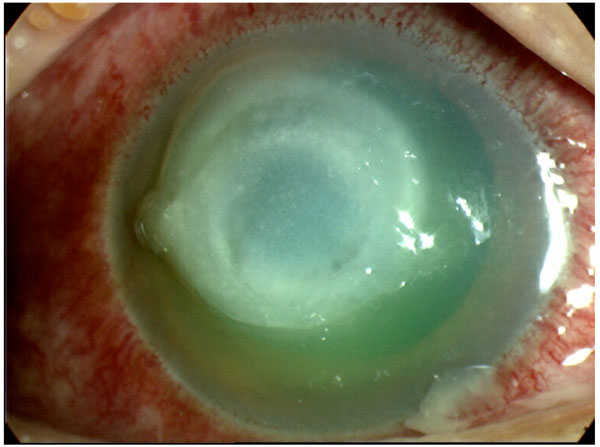
Bacterial keratitis due to Pseudomonas spp.
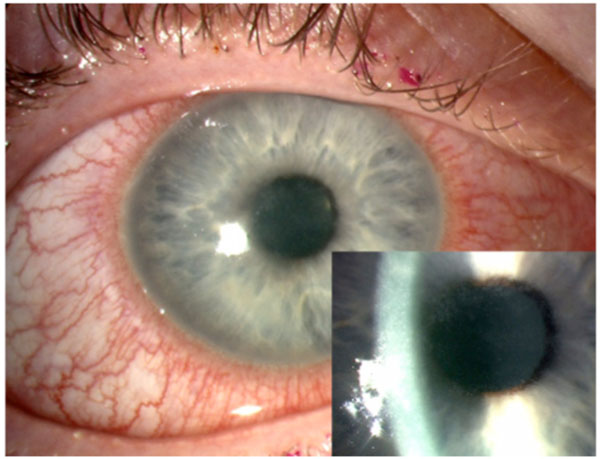
Acanthamoeba keratitis, Insert: higher magnification showing epithelial irregularity in early acanthamoeba keratitis.
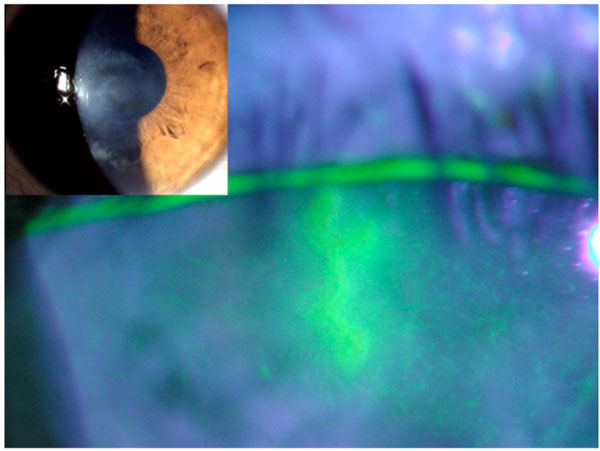
A dendritic ulcer from herpes simplex keratitis stained with fluorescein and viewed with a cobalt blue light. Insert: appearance in natural light.
In total, 49 families were identified in fungal keratitis, with 2 being yeast and 47 filamentous (Table 1) while 25 families of bacteria were identified; of which 12 were Gram positive and 13 Gram negative (Table 2). In amoebic keratitis, 3 families, predominantly Acanthamoebidae, were identified (Table 5); while in viral keratitis the majority of reports were from the Herpesviridae family (Table 6). Risk factors and treatment for each type of keratitis were also identified in the review. The clinical symptoms of keratitis are similar despite the infectious agent and is characterised by local pain, lacrimation, and photophobia, however the clinical appearance of lesions can differ depending upon organism [10].
Number of Identified Families Implicated in Fungal Keratitis
| Phylum | Number of Identified Families | |
|---|---|---|
| Mycota | Ascomyctoa | 38 |
| Basididiomycota | 7 | |
| Zygomycota | 2 | |
| Slime Mold | Myxomycota | 1 |
| Straminipila | Oomycota | 1 |
Number of Identified Families Implicated in Bacterial Keratitis
| Phylum/Division | Number of Identified Families | |
|---|---|---|
| Gram positive | Actinobacteria | 7 |
| Firmicutes | 5 | |
| Gram negative | Proteobacteria | 12 |
| Bacteroides | 1 | |
| Gram variable | n/a | 0 |
Diversity of Fungal Species Implicated in Keratitis (1Previously Cephalosporium spp., 2Previously Monilia spp. - Species Not Identified)
| Family | Genus | Species | References |
|---|---|---|---|
| Arthrodermataceae | Microsporum | - | [32] |
| Bionectriaceae | Gliocladium | - | [13] |
| Botryosphaeriaceae | Diplodia | - | [89] |
| Lasiodiplodia | theobromiae | [17, 60, 90] | |
| Phoma | eupyrena | [91] | |
| Ceratobsidiaceae | Rhizoctonia | - | [13] |
| Chaetomiaceae | Chaetomium |
- atrobrunneum |
[78, 92, 101, 102] |
| Chaetosphaeriaceae | Diplosporium | - | [103] |
| Gongromeriza | [13] | ||
| Trichothecium | - | [13, 104] | |
| Clavicipitaceae | Beauveria | bassiana | [13, 105] |
| Metarhizium | - | [24] | |
| Cordycipitaceae | Acrostalagmus | cinnabarensis | [106] |
| Corticiaceae | Sporotrichum | schenekii | [52, 106] |
| Cunninghamellaceae | Cunninghamella | - | [13] |
| Cystofilobasidiaceae | Guehomyces | pullulans | [24] |
| Davidiellaceae | Cladosporium | - | [55, 107, 108] |
| Dermateaceae | Gloeosporium | fructigenum | [88] |
| Dothioraceae | Aureobasidium | pullulans | [16, 109, 110] |
| Pyrenochaeta | - | [13] | |
| Endomycetaceae | Geotrichum | candidum | [13, 111] |
| Eremomycetaceae | Arthrographis | kalrae | [88] |
| Filobasidiaceae | Blastomyces | dermatidis | [106] |
| Exsophiala | jeanselmei | [112, 113] | |
| Herpotrichiellaceae | Fonsecaea | pedrosoi | [33, 114] |
| Phialophora | pedrosoi | [13, 115] | |
| verrucosa | |||
| Pullularia | - | [104] | |
| Torula | - | [16] | |
| Wangiella | dermatides | [24] | |
| Hypocreaceae | Acremonium1. | potronii | [17, 106, 116, 117] |
| Acrostalagmus | cinnabarensis | [106] | |
| Gliocladium | - | [13] | |
| Sepedonium | - | [13] | |
| Trichoderma | - | [13, 24] | |
| Hyponectriaceae | Humicola | - | [16] |
| Glomerallales | Colletotrichum | denatium | [118-120] |
| gleosporiodes | |||
| graminicola | |||
| Gymnoascaceae | Gymnoascus | - | [110] |
| Incertae sedis | Scytalidium | hyalinum | [112] |
| Myrothecium | - | [111] | |
| Lasiosphaeriaceae | Monotospora | - | [13] |
| Lophiostomataceae | Tetrapola | - | [121] |
| Metacapnodiaceae | Hormiscium | - | [13] |
| Microascaceae | Doratomyces | - | [13] |
| Monosporium | - | [108] | |
| Pseudoallescheria | boydii | [32, 89, 112] | |
| Scedosporium | apiospermum | [47, 78, 107] | |
| prolificans | |||
| Scopularisopsis | blochi | [13, 21, 106] | |
| brevicaulis | |||
| Mucoraceae | Mucor | cornealis | [32, 106] |
| racemosus | |||
| Rhizopus | nigricans | [103, 106, 108] | |
| parasiticus | |||
| Zygorhynchus | - | [13] | |
| Mycospaerellaceae | Cercospora | - | [13] |
| Hormodendrum | - | [82, 103] | |
| Nectricaceae | Bactridium | - | [13] |
| Cylindrocarpon | lichenicola | [89] | |
| Fusarium | avenascus | [13, 17, 21, 32, 47, 90, 93, 106, 122-125] | |
| dimerum | |||
| episphaeria | |||
| moniliforme | |||
| nivale | |||
| oxysporum | |||
| poae | |||
| solani | |||
| sporotrichioides | |||
| subglutinans | |||
| verticilloides | |||
| Fusidium | terricola | [106] | |
| Fusoma | - | [13] | |
| Gibberalla | fuzikuroi | [106] | |
| Moniliaceae | - | [122] | |
| Volutella | - | [17, 111] | |
| Niessliaceae | Stachybotrys | - | [13] |
| Ophiostomatales | Sporothrix | schenckii | [100] |
| Onygenaceae | Chrysosporium | - | [107] |
| Orbiliaceae | Arthrobotrys | oligospora | [126] |
| Phycomycetaceae | Periconia | Keratidis | [106] |
| Plectosphaerellaceae | Verticillium | - | [78] |
| Pleosporaceae | Alternaria | alternata | [127] |
| Bipolaris | australiensis | [33, 83, 127] | |
| hawaiiensis | |||
| spicefera | |||
| Brachysporium | - | [78] | |
| Curvularia | brachyspora | [115, 121, 127-135] | |
| fallax | |||
| geniculata | |||
| lunata | |||
| pallescens | |||
| prasadii | |||
| senegalensis | |||
| verruculosa | |||
| Dreschlera | halodes | [82, 115] | |
| Exserohilum (Setosphaeria) | roseum | [83, 89, 117, 125] | |
| rostratum | |||
| solani | |||
| Helminthosporium | - | [78, 82] | |
| Stemphylium | - | [13] | |
| Pyllachoraceae | Colleotrichum | atramentum | [111] |
| Pythiaceae | Pythium | insidiosum | [101, 112] |
| Saccharomycetaceae | Candida2. | albicans | [21, 24, 47, 49, 88, 113, 116, 125, 136-139] |
| curvata | |||
| humicola | |||
| glabrata | |||
| guilliermondii | |||
| lipolytica | |||
| parapsilosis | |||
| tropicalis | |||
| zeylanoides | |||
| Saccharomyces | - | [13, 109] | |
| Sclerotiniaceae | Botrytis | - | [106] |
| Sordariaceae | Chrysonilia | sitophila | [101] |
| Sporidiobolaceae | Rhodotorula | glutinis | [140, 141] |
| minuta | |||
| Syncephalastraceae | Syncephalastrom | - | [82] |
| Tremellaceae | Cryptococcus | laurentii | [18, 24, 116] |
| neoformans | |||
| Trichocomaceae | Aspergillus | alternata | [13, 83, 91, 94, 110, 122, 123, 125, 128, 130, 138, 142] |
| flavus | |||
| fumigatus | |||
| glaucus | |||
| nidulans | |||
| niger | |||
| oryzae | |||
| terreus | |||
| versicolour | |||
| Penicillium | citrinum | [32, 106, 143] | |
| crustaceum | |||
| expansum | |||
| spinulosum | |||
| Paecilomyces | farinosus | [113, 144, 145] | |
| lilacinus | |||
| Trichosphaeriaceae | Khuskia | - | [90] |
| Trichosporonaceae | Trichosporon | beigelii | [90, 95, 106, 140] |
| capitatum | |||
| rugosum | |||
| Venturiaceae | Fusicladium | - | [13] |
| n/a | Cephaliophora | - | [13] |
| Dichotomophthoropsis | - | [90, 146] | |
| Mycelia | sterilia | [13, 88, 109] |
Diversity of Bacterial Species Implicated in Keratitis, (- Species Not Identified)
| Family | Genus | Species | References |
|---|---|---|---|
| Actinomycetaceae | Actinomyces | bovis | [106] |
| Aeromonadaceae | Aeromonas | hydrophilia | [37] |
| Alcaligenaceae | Achromobacter | - | [10, 147] |
| Alcaligenes | faecalis | [40, 148] | |
| Bacillaceae | Bacillus | cefilius | [130, 149] |
| subtilis | |||
| Burkholderiaceae | Burkholderia | cepacia | [94, 150] |
| Clostridiaceae | Peptostreptococcus | micros | [131] |
| Sarcina | - | [111] | |
| Comamonadaceae | Comamonas | acidovorans | [94] |
| Corynebacteriaceae | Corynebacterium | diptheriae | [14, 91, 92, 130, 151] |
| hofmannii | |||
| minutissimum | |||
| pyogenes | |||
| xerosis | |||
| Enterobacteriaceae | Citrobacter | diversus | [47, 152] |
| freundic | |||
| Enterobacter | aerogenes | [37, 138, 140, 152] | |
| cloacae | |||
| Escherichia | coli | [108, 151] | |
| Hafnia | alvei | [147] | |
| Klebsiella | oxytoca | [93, 138, 152, 153] | |
| ozaenae | |||
| pneumonia | |||
| Morganella | morganii | [34, 113] | |
| Pantoea | agglomerans | [96] | |
| Proteus | mirabilis | [108, 152, 153] | |
| vulgaris | |||
| Providencia | - | [113] | |
| Serratia | liguefaciens | [34, 40, 124, 151] | |
| marcescens | |||
| Enterococcaceae | Enterococcus | faecalis | [93, 138] |
| Flavobacteriaceae | Capnocytophaga | - | [154] |
| Flavobacterium | meningosepticum | [94] | |
| Chryseoacterium | - | [113] | |
| Micrococcaceae | Micrococcus | - | [83, 135] |
| Moraxellaceae | Acinetobacter | baumannii | [37, 94, 135, 140] |
| calcoaceticus | |||
| Moraxella | catarrhalis | [34, 79, 130, 147] | |
| launata | |||
| Mycobacteriaceae | Mycobacteria | abscessus | [10, 94, 113] |
| chelinae | |||
| fotuitum | |||
| Neisseriaceae | Eikenella | corrodens | [10] |
| Kingella | denitrificans | [10] | |
| Neisseria | gonorrhoea | [113, 123, 152] | |
| meningitides | |||
| Nocardiaceae | Nocardia | asteroides | [152, 155] |
| Pasteurellaceae | Haemophilus | aegyticus | [124, 152, 156] |
| influenza | |||
| parainfluenza | |||
| Peptococcaceae | Peptococcus | prevotii | [14, 91] |
| Propionibacteriaceae | Propionibacterium | acnes | [2, 94] |
| Pseudomonadaceae | Pseudomonas | acidovorans | [14, 34, 79, 138, 140, 146, 147] |
| aeruginosa | |||
| cepacia | |||
| fluorescens | |||
| maltphilia | |||
| oryzihabitans | |||
| Staphylococcaceae | Staphylococcus | aureus | [40, 93, 108, 148] |
| epidermidis | |||
| coagulase negative | |||
| Streptococcaceae | Streptococcus | dysgalactie | [10, 34, 40, 93, 94, 96, 131, 135, 140, 157] |
| mitis | |||
| morbillorum | |||
| oralis | |||
| parasanguis | |||
| pyogenes | |||
| salivarius | |||
| sanguinis | |||
| viridans | |||
| Streptomycetaceae | Streptomyces | - | [104] |
| Vibrionaceae | Vibrio | vulnificus | [158, 159] |
| Xanthomonadaceae | Stenotrophomonas | maltophilia | [37, 140, 150, 151] |
| Xanthomonas | - | [157] |
List of Microorganisms Identified as the Infectious Agent in Conditions of Amoebic Keratitis, (- Species Not Identified)
List of Microorganisms Identified as the Infectious Agents in Conditions of Viral Keratitis
Summary of the Most Common Risk Factors Associated with Keratitis
| Risk Factors | Commonly Associated Microorganisms | References |
|---|---|---|
| Ocular Trauma | Fungal, i.e. Fusarium spp | [11, 83] |
| Use of Contact Lenses | Bacterial, i.e. Pseudomonas aeruginosa | [34, 78] |
| Ocular Surface Disease | Yeast infections, i.e. Candida albicans | [18] |
| Systemic Disease | Opportunistic organisms | [88] |
| Use of Corticosteroids | All | [86, 87, 167] |
Fungal Keratitis
Mycotic keratitis, due to filamentary fungi, is typified by a grey-white infiltrate with irregular feathery margins and raised borders (Fig. 2a); along with suppuration, hypopyon, satellite lesions, Descemet’s fold, and an immune ring with minimal surrounding infiltrate [11]. Filamentous fungi such as Fusarium spp and Aspergillus spp are common in mycotic keratitis. However, aetiologies exhibited by unicellular fungi, such as yeasts of the Saccharomycetaceae and Tremellaceae families, are often clinically similar to those of bacterial keratitis (Fig. 2b) [12].
The majority of the identified organisms were ‘true fungi’ or Mycota; of 48 families identified, only 2 were not of this classification (Table 3). Cunninghamellaceae is a slime mold from the phylum Myxomycota and was reported by Wang et al. in 2009 from patients in central China [13]. Pythiaceae from the Straminipila, phylum Oomycota was reported by Sirikul et al. in 2008 from patients in Thailand [14]. From those within Mycota, the majority were of the phylum Ascomycota (Table 3).
Geographical location and climate are reported to influence the clinical presentation and outcome of fungal diseases, probably through changes in the causative agent [15]. Fusarium solani ocular infections are reported to have the most severe prognosis; its progression is comparatively rapid with patients demonstrating corneal perforation in only a few weeks [11]. In contrast, dematiaceous fungi such as Curvularia and Lasiodiplodia tend to result in persistent low-grade infection and may present with a slightly pigmented lesion [16, 17].
A range of treatments have been suggested for use in mycotic keratitis including natamycin [18-20], azoles such as fluconazole [21, 22] and voriconazole [23], and amphotericin B [18, 24]. Kalavathy et al. [25] reported that the use of the antifungal natamycin (5%) topically was the most ideal treatment available against filamentous fungi especially Fusarium spp. However the molecular weight of natamycin is relatively high (665.73 g.mol-1) and as a consequence it has low penetration into corneal tissue [26]. This may explain the reduced effectiveness of natamycin in treating deep mycosis as observed by Senupta et al. [27]. Galarreta et al. [21] has reported intensive use of topical econazole (1%) to have efficacy against filamentary fungi such as Fusarium spp. While fluconazole has been used to treat yeast infections with significant results, Galarreta et al. [21] reports poor outcomes in treating filamentary fungi. The use of amphotericin B was prevalent in the past as a treatment for mycotic keratitis, especially caused by yeast; although a very effective treatment there are significant side effects associated with its use [28]. Hence, the use of amphotericin B as an initial treatment has significantly declined, but it may still be implemented as a secondary measure [29]. Recently, the clinical use of voriconazole has increased. It can be administered topically or systemically, and achieves high penetration into the cornea [23]. Clinically, voriconazole has been reported to be an effective treatment for mycotic keratitis [30, 31].
Although topical treatments with antifungal agents are moderately effective against either yeasts or filamentous fungi, they are by no means the optimal therapy due to their reduced corneal perforation. Systemic antifungals are typically given, along with topical therapy, particularly for deep infections and those close to the vascularised corneal limbus. If medical therapy fails then surgical invention is required. Xie et al. [32] reported that surgery was performed in 92.4% of patients with fungal keratitis, with only 7.6% controlled by topical mediations. Furthermore Saha et al. [33] reported that 59.4% of the patients required surgery, due to ineffective medical therapy.
Bacterial Keratitis
Bacterial keratitis commonly presents with an overlying epithelial defect and relatively less distinct cellular infiltrate and suppuration than fungal keratitis (Fig. 3). In addition, progression of bacterial infection tends to be slower than ophthalmic mycoses [34]. However Pseudomonas keratitis, most commonly occurring in association with contact lens wear, can progress rapidly and is identified by a considerable suppurative infiltrate and the presence of Gram-negative organisms [34].
Similar to fungal keratitis, the severity of bacterial infections is largely dependent upon the causative agent. Staphylococcus epidermidis [35], Streptococcus pneumoniae and Pseudomonas aeruginosa [36] are reported to be the most common pathogens associated with bacterial keratitis. Corneal infection with these pathogens can be quite severe; Kaye et al. [37] reported that the presence of S. pneumoniae was more often associated with permanent damage to the eye and P. aeruginosa infection has been found to progress rapidly to corneal perforation even with the rigorous use of antibiotics [38].
Of the 25 identified families, the distribution between Gram positive and Gram negative organisms is relatively even. However, apart from one family, Flavobacteriaceae, in the phylum Bacteroides, all other identified Gram negative organisms are from the phylum Proteobacteria (Table 4).
In the past 20 years fluoroquinolones such as ofloxacin and ciprofloxacin have been used as the primary treatment for bacterial keratitis [39]. More recently it has been suggested that the monotherapeutic use of fluoroquinolones in treating bacterial keratitis may have led to the development of resistance against the drug [7]. However there are conflicting reports regarding this issue. For example, Schaefer et al. [40] reported that most Gram negative and Gram positive bacteria were sensitive to fluoroquinolones, with the exception of some S. pneumoniae and Pseudomonas cases which remained resistant. Jhanji et al. [41] reported S. epidermidis isolated from an infected cornea was resistant to all fluoroquinolones used. In contrast, Shalchi et al. [42] has claimed no increasing resistance to fluoroquinolones and advised their continued use. It is also thought that systemic use of fluoroquinolones, rather than topical, may be responsible for resistance. Furthermore, Reviglio et al. suggests that topical application of fluroquinones promotes the expression of corneal metalloproteinases, the proteolytic properties of which can adversely affect the wound healing process [43].
It is important to note in treating keratitis that in vitro susceptibility testing rarely corresponds to the clinical reality [44, 45], as difficulties in regulating doses of topical treatments within the eye [46] and inaccurate breakpoints are used in in vitro susceptibility testing [37]. As the breakpoints being currently used assess the systemic administration of antibiotics as opposed to ocular topical administration, the resistance in ocular infections may be overestimated [37, 47].
Amoebic Keratitis
Acanthamoeba is a ubiquitous protozoan that can be largely found in soil and water in two stages of its lifecycle, the trophozoite (proliferative) stage or cyst stage [48]. Amoebic keratitis is closely associated with contact lens wear, with approximately 83% of cases occurring in lens users. In non-lens wearers it is usually a consequence of ocular trauma and exposure to contaminated water or soil, often in agricultural workers [51]. Amoebic keratitis has also been reported after surgical trauma including penetrating keratoplasty (PK) and radial keratotomy (RK) procedures [51].
Acanthamoeba are capable of causing permanent visual impairment if not diagnosed and treated quickly [49, 50]. Diagnosed early, treatment with anti-amoebic therapy is generally successful [51]. A poor prognosis is associated with a delay in diagnosis [51]. While the commonly termed Acanthamoeba is the most studied agent of this type in keratitis, it is not the only amoebic infection that has been identified. Members of Vahlkampfia [52], Paravahlkampfia [53] and Hartmannella [54] species have also been identified in cases of amoebic keratitis (Table 5).
While treatment generally is successful, in unfavourable conditions Acanthamoeba have been known to invade and produce cysts that prolong their life-span. They have been shown to remain dormant for up to a year, before activation occurs, and they return to being trophozoites [49]. Further, topical steroids given to reduce inflammation have been shown to cause encystment and even promote amoebic proliferation [55].
The most common treatment for amoebic keratitis is chlorhexidine or combination therapy using polyhexamethylene biguanide (PHMB) and a diamadine such as propamidine isethionate [56]. Kosrirukvongs et al. [56] compared the efficacy of these treatments and reported that the use of such combination therapy resulted in better visual acuity for the patients. Narasimhan et al. [57] showed that the use of PHMB was more successful against trophozoites in vitro. Diamidines have been shown to be successful against both the trophozoite and cyst forms [51].
Acanthamoebic keratitis is most commonly identified in its early stages by dendritiform epithelial pattern, small white infiltrates and radial keratoneuritis. Fig. (4) shows epithelial irregularity in early acanthamoeba keratitis [58, 59]. As the infection progresses, it can take up to 3 months for the classic ring-shaped cellular infiltrate to form, however this indication is unreliable for early instigation of treatment [60]. Corneal suppuration, abscess formation, chorioretinitis and chronic immune-mediated scleritis have been reported with the progression of acanthamoebic keratitis [49].
Viral Keratitis
Herpes Simplex Virus keratitis is the most common cause of irreversible blindness in developed countries. Worldwide, an estimated 10 million persons suffer from herpetic keratitis, with about 2 million individuals left with impaired vision [61-63]. Although Herpes Simplex Virus-Type 1 (HSV-1) is the most common cause of viral keratitis, it is not the only implicated viral pathogen. Varicella Zoster Virus, also a member of the Herpes viridae family, has been identified as a causal agent in a select few cases, while the Vaccinia virus has been identified as the result of an adverse reaction to the small pox immunisation (Table 6) [64-66].
With a seroprevalence of HSV-1 as high as 76%, the Herpetic Eye Disease Study (HEDS) found a recurrence rate of approximately 34% [67, 68]. HSV are reported to frequently reside within neural cells, where they can become latent [69]. Clinically, it has been suggested that the dendritic patterns common in HSV-1 keratitis mirror the patterns of the subbasal nerve plexus present in the corneal epithelium [70], indicating the migration of the virus into neural cells. Latency in neural crest cells is thought to explain the high incidence recurrence.
Primary HSV keratitis is clinically characterised by a dendritic lesion which has a morphological branching pattern across the cornea [71]. Recurrent disease is characterised by followed by corneal scarring, thinning, and vascularisation [72] (Fig. 5). The early stages of HSV-1 infection closely correspond to the clinical presentation of Acanthamoebic keratitis.
Acyclovir is the accepted primary treatment for herpetic keratitis. Acyclovir is a deoxyguanosine analogue, and post-phosphorylation it is a potent inhibitor of viral DNA polymerase; however, there are reports of growing resistance to acyclovir [73]. Resistance to deoxyguanosine analogues can develop through mutation of the viral gene thymidine kinase, which is essential for the phosphorylation of acyclovir. However, not all prescribed medication requires thymidine kinase for activity and consequently resistance is mostly acyclovir specific. In contrast, resistance that arises through mutation of the viral DNA polymerase can influences a wide range of anti-viral drugs [73, 74]. Wilhelmus [63] has conducted an extensive review on the quality and efficacy of the currently prescribed anti-viral topical treatments [63, 75]. Corneal graft surgery in patients with HSK has been associated with recurrence of infection and is often avoided unless needed to manage a corneal perforation [76].
Keratitis Risk Factors
Microbial keratitis usually occurs in conjunction with specific risk factors [77]. The most common of which are the use of contact lenses, corneal trauma, or underlying ocular surface disease (Table 7). Recent work by Shah et al. suggests statistically significant relationships between gross national income and fungal or bacterial keratitis with the former more prevalent in developing nations [6].
The use of contact lenses has been closely associated with an increased incidence of bacterial keratitis [34]. Pseudomonas aeruginosa and Staphylococcal species are some of the most common organisms cultured in contact lens associated bacterial keratitis [78]. Development of hydrogel day and night wear contact lenses coupled with greater comfort, leading to longer wearing times, and fashion trends for coloured contact lenses without refractive correction, saw an increase in contact lens use and misuse, with an initial increase in ocular infections [79]. A recent study by Stapleton and coworkers indicated that overnight wear of contact lenses, despite the introduction of silicone hydrogel materials that decrease hypoxia compared to hydrogel lens types, still has an increased incidence of infection compared to daily wear [124]. Contact lenses can serve as a platform for the microbial proliferation, encouraging microbial adhesion to the cornea. Korb et al. [77] have suggested that the use of contact lenses can also interfere with the ocular defences, by leading to hypoxia and/or disruption of the epithelial-tear film interactions, a view supported by others such as McNarma et al. [80] and Thakur and Wilcox [81].
Direct corneal damage disrupts the innate immune system of the eye, enabling entry by microbes into the abrasion and consequent infection. Trauma is quite commonly associated with infection by filamentous fungi such as Fusarium solani, Aspergillus spp and Bipolaris spp; especially when the trauma is caused by vegetative matter particularly in tropical climates [82, 83]. It is most likely that the vegetative material was previously colonised by the microorganisms, and consequently injury and infection occurs almost simultaneously [11].
Corneal surgery is a risk factor for microbial keratitis as the corneal epithelial barrier is breached [11]. Due to the immune-privileged nature of the eye, any break in the corneal epithelium renders the eye susceptible to infection. Furthermore, post-operative care usually requires the use of topical steroids to control the immune response. The prophylactic use of corticosteroids has become quite controversial and has been associated with an increase in microbial growth and keratitis [84]. A number of reports have suggested that corticosteroids may either facilitate an increase in microbial proliferation and/or possibly impair the ocular immune response thus encouraging microbial infection [85-87].
Local weakening of the immune defences is the most common predisposing factor associated with keratitis caused by opportunistic infections, such as by Candida albicans or other yeast fungi [18]. In contrast, systemic immune systems affected by diseases such as diabetes mellitus and HIV infection are associated with a great range of opportunistic infections [88]. It is also possible for keratitis to develop as a result of endogenous infections, typically by Gram positive bacteria such as Staphylococcus spp. [5].
CONCLUSIONS
Keratitis is a serious infection of the eye and contributes to one of the leading causes of monocular blindness worldwide. Whilst statistics are difficult to obtain, there is evidence of regional variability in both incidence and type of infection [5, 58, 89-96]. For example, contact lens related bacterial keratitis is more prevalent in developed countries whereas fungal keratitis is a major blinding disease in more tropical climates [27, 97, 98].
This review has revealed 232 species reported to be infectious agents in keratitis and can act as a resource to clinicians and researchers for initial information on species. However, identification of species associated with microbial keratitis is relatively complex; [10] microbiological sampling does not always yield a result and different micro-organisms can produce a similar clinical picture [11, 60]. Furthermore, few clinical signs are pathgnonomic for the type of infection; for example: perineural infiltrates are virtually pathgnomonic for Acanthamoeba infection [51] however they have also been reported in bacterial keratitis [99]. Thus, improved diagnostic techniques, such as polymerase chain reaction (PCR), are clearly needed for routine use in cases of microbial keratitis to rapidly identify the infectious agent and permitting targeted therapy.
Current treatment for microbial keratitis involves an intensive regime of topical therapy, with significant morbidity and inconvenience for the patient, such that treatments available for microbial keratitis need to be improved [32, 37, 98]. However, despite previous efforts in designing solid drug delivery systems, the most popular and accepted forms of antibiotics for local delivery remain as liquid or gel forms for topical administration. In the eye, antibiotics delivered as eye drops suffer rapid and extensive pre-corneal loss caused by drainage and high tear turnover; typically less than 5% of applied drug penetrates the cornea and reaches intra-ocular tissues [8]; thus, appropriate dosing is difficult [100]. Furthermore, there is a distinct lack of information concerning the pathogenesis of how the different types of microbial keratitis develop and the host factor involved. Advances in our knowledge of keratitis, in particular data on the causal organisms, will facilitate the development of more specific and effective treatments as well as techniques to prevent infection.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
The authors acknowledge the support of grants from the Ophthalmic Research Institute of Australia (ORIA) and the National Health and Medical Research Council (NHMRC, APP630510) to Foster and Watson.

