All published articles of this journal are available on ScienceDirect.

Abnormalities of Fundus Autofluorescence in Pigmented Paravenous Chorioretinal Atrophy
Abstract
The aim of this study is to investigate fundus autofluorescence (FAF) as well as fluorescein angiography (FA), indocyanine green angiography (IA), and optical coherence tomography (OCT) in a patient with pigmented paravenous chorioretinal atrophy (PPCRA). A funduscopic examination revealed chorioretinal atrophy along the paravenous area in both eyes. A marked bone spicule pigment clumping together with the atrophy was noted left eye. FA and IA showed a window defect and hypofluorescence, respectively, which exclusively corresponds to the atrophic area along the retinal vein area and the optic disc both eyes. FAF revealed geographic hypofluorescence along the paravenous and supranasal retinal areas. Hyperfluorescence was noted, which comparatively surrounded the hypofluorescence in the peripheral paravenous distribution. Hypofluorescence detected by FAF corresponded to the areas of retinal thinning and atrophy detected by OCT and FA. FAF is a useful examination in PPCRA, which can noninvasively demonstrate the distribution of deficit and dysfunction of retinal pigment epithelium.
INTRODUCTION
Pigmented paravenous chorioretinal atrophy (PPCRA) was described as retino-choroiditis radiata in 1937 [1]. PPCRA is a bilaterally symmetrical stationary disease of the ocular fundus, presenting bone spicule pigment clumping in paravenous distributions and areas of atrophy surrounding the optic disc. In most cases, fundus abnormality is initially noted on a routine examination.
Fundus autofluorescence (FAF) displays lipofuscin at the level of the retinal pigment epithelium (RPE), which is considered a useful method to detect early RPE alternations. FAF has demonstrated specific RPE abnormalities in various fundus disorders such as age-related macular degeneration, Stargardt disease, retinitis pigmentosa (RP), and acute zonal occult outer retinopathy (AZOOR) [2-5]. However, there are no reports on PPCRA showing FAF findings in detail.
We herein report a case of PPCRA in a Japanese female, who underwent FAF as well as fluorescein angiography (FA), indocyanine green angiography (IA), and optical coherence tomography (OCT).
REPORT OF A CASE
A 59-year-old female presented with fundus abnormalities on a medical examination without ocular symptoms in both eyes 14 years ago. She was referred to our hospital for further follow-up of the fundus abnormalities on October 8, 2010. Her visual acuity was 1.2 both eyes with no major refractive error. Anterior segments and vitreous media were normal. A funduscopic examination revealed chorioretinal atrophy along the paravenous area in both eyes, and supranasal retinal areas in her left eye without macular involvement. A marked bone spicule pigment clumping together with the atrophy was noted left eye (Fig.1A,B). FAF revealed geographic hypofluorescence along the paravenous and supranasal retinal areas. Linear hyperfluorescence was noted, which comparatively surrounded the hypofluorescence in the peripheral paravenous distribution (Fig. 1C,D). FA and IA showed a window defect (Fig. 2A,B), and hypofluorescence (Fig.2C,D), respectively, which exclusively corresponds to the atrophic area along the retinal vein area and the optic disc both eyes. The patient was diagnosed with PPCRA. Spectral domain OCT (RS-3000 advance®; NIDEK, Gamagori, Japan) displayed thinning of the retina in macular map and cross scans in the atrophic areas revealed thinning of not only RPE layer and the outer retinal layer, but also inner retinal layer (Fig. 3A,B). Enhanced depth imaging OCT scans demonstrated that choroidal thickness was thin in the areas (Fig. 3C-F). The Humphrey SITA-Standard 30-2 visual field test showed scotomata corresponding to the retinal atrophic area both eyes. An electroretinogram (ERG) demonstrated that right eye was subnormal, while reduced a and b waves response was noted in left eye together (Fig. 4) with more extensive atrophy. Fundus findings and visual field defects remained unchanged during these 14 years.
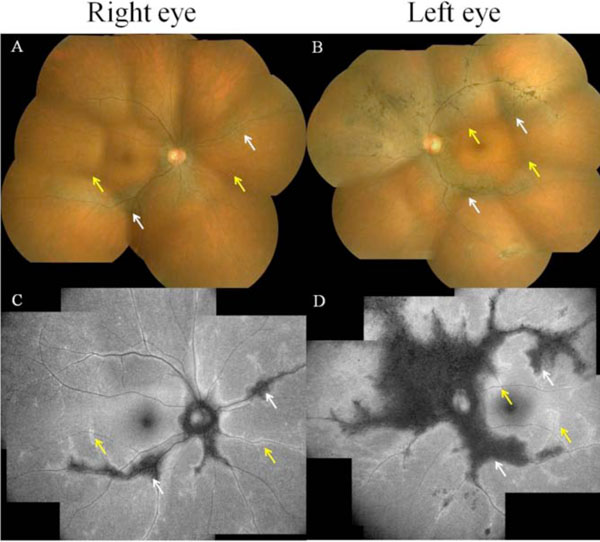
A funduscopic examination reveals chorioretinal atrophy along the paravenous area in both eyes and supranasal retinal areas left eye without macular involvement. Note also a marked bone spicule pigment clumping together with the atrophy of the left eye (A, B). Fundus autofluorescence examination reveals geographic hypofluorescence (C, D; white arrows) along the paravenous and supranasal retinal areas. Hyperfluorescence surrounding the hypofluorescence in the peripheral paravenous distribution (C, D; yellow arrows). These arrows are corresponding to those shown in fundus examination.
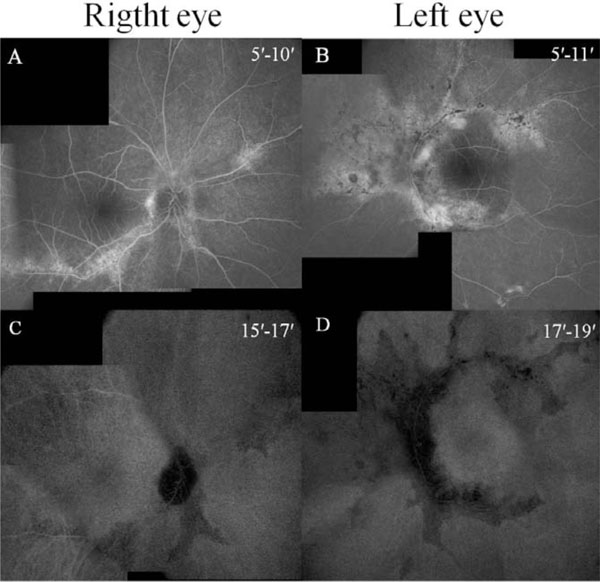
Fluorescein angiography shows a window defect (A, B) and indocyanine green angiography shows hypofluorescence (C, D) corresponding to the atrophy.
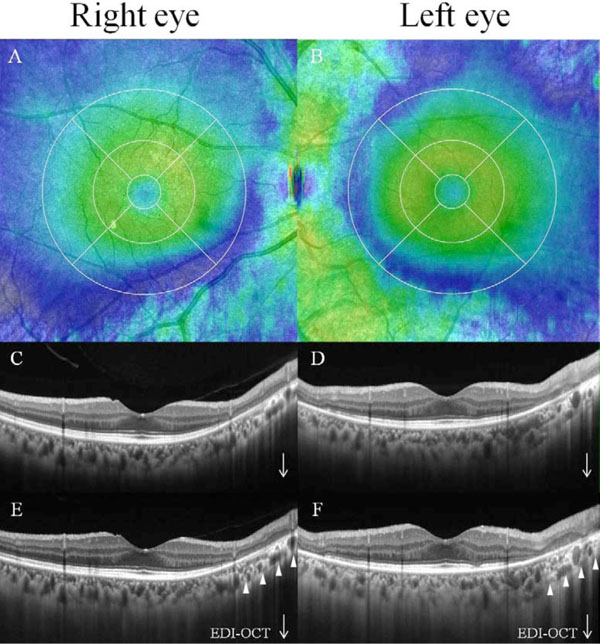
Blue area of the color map reveals thinning of the retina on optical coherence tomography (OCT) in macular map mode (A, B). Cross scans in the atrophic areas revealed thinning of not only RPE layer and the outer retinal layer, but also inner retinal layer (C, D). Enhanced depth imaging OCT scans demonstrated that choroidal thickness was thin (arrowheads).

An electroretinogram demonstrated that right eye was subnormal, while reduced a and b waves response was noted in left eye together with more extensive atrophy.
DISCUSSION
FA and IA showed window defects and hypofluorescence in the atrophic area, respectively, which were almost the same areas. However, FAF clearly demonstrated characteristic
hypofluorescence, simulating hyperfluorescence in the paravenous area in this case. Hypofluorescence in FAF shows the atrophy or disappearance of RPE, because of a loss of lipofuscin in RPE [6]. Indeed, hypofluorescence detected by FAF corresponded to the areas of retinal thinning and atrophy detected using FA, IA, and OCT. In contrast, hyperfluorescence shows dysfunction of RPE that accumulates lipofuscin in RPE, suggesting the possibility of RPE atrophy in the future [6]. This case presented a novel FAF findings presenting hyperfluorescence, which comparatively surrounded the hypofluorescence in the peripheral paravenous distribution. These results indicates that dysfunction of RPE takes place more extensively on the fundus than the chorioretinal lesions detected by FA and IA. Therefore, dysfunction of RPE might be closely associated with the retinal atrophy and subsequent visual field defect in PPCRA.
Although the pathogenesis of PPCRA is still unknown, FAF extensively revealed abnormalities of the RPE correlated with paravenous regions. In addition, other ophthalmological examinations showed thinning of choroidal thickness and atrophy of the choroid together with the paravenous atrophy. Therefore, choroidal circulation disorder in the paravenous region of the retina may contribute to RPE abnormalities, which plays a potential role in the pathogenesis of PPCRA.
As differential diagnoses, AZOOR and RP can show similar fundus findings with PPCRA, together with hypofluorescence displayed by FAF. However, unlike this case, loss of visual acuity and photopsia within the scotomata are common ocular symptoms associated with AZOOR patients, and night blindness and progressive visual field loss are observed in RP patients, respectively. FAF shows diffuse hypofluorescence around the optic disc in AZOOR [5], and high density rings of FAF imaging in RP [4], although PPCRA characteristically shows hypofluorescence along the paravenous area.
Usually, the amplitude of the ERG is markedly reduced or disappears from early phase of RP. In this case, right eye was subnormal, while reduced a and b waves response was noted in left eye together with more extensive atrophy. When the atrophy involves extensive areas, the amplitude should be reduced even in PPCRA. Therefore, it may be difficult to differentiate PPCRA from RP based on only the ERG findings in selected cases.
In conclusion, FAF can noninvasively and clearly demonstrate the distribution of deficit and dysfunction of RPE. Also, FAF more extensively revealed abnormalities compared with FA or IA, which is a useful examination to compliment a diagnosis of PPCRA.
ACKNOWLEDGEMENTS
Declared none.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.

